Antepartum Fetal Surveillance
Table of Contents:
©2019 BoardsMD
This can be a pretty challenging topic at the medical student level, and it is often very poorly taught and very poorly organized in other lecture series.
We are going to completely demystify and break down the various modalities that we have at our disposal when it comes to fetal surveillance.
Fundus Landmarks
One very high yield pearl that is especially useful in the context of exam questions is having the ability to compare the fundal height to the gestational age.
In the STEM of a given patient vignette, they will often tell you, the number of weeks gestational age of the patient in question.
We can then compare that patients reported gestational age with the height of their fundus and see if there is a correlation or concordance between the two.
In an ideal or normal scenario If we were to have a patient who is currently at 20 weeks gestational age, then we would expect that their fundal height would be approximately the same number. In this case, 20 centimeters.
By comparing the gestational age in number of weeks to the fundal height in centimeters, we can determine whether the fundal height is short or large relative to the gestational age.
Patient vignettes in question stems will often use specific code words in order to give you a hint as to the fundal height.
For example, if a board vignette tells you that the fundus is at the level of the umbilicus, then this is really telling you that the fundal height is equivalent to 20 weeks gestation.
If the question States that the fundus is between the umbilicus and the pubic synthesis, this is really telling you that the fundal height is consistent with 16 weeks gestation.
If the fundus is at the level of the pubic symphysis, then this is suggesting that the fundal height is consistent with the gestational age of 12 weeks.
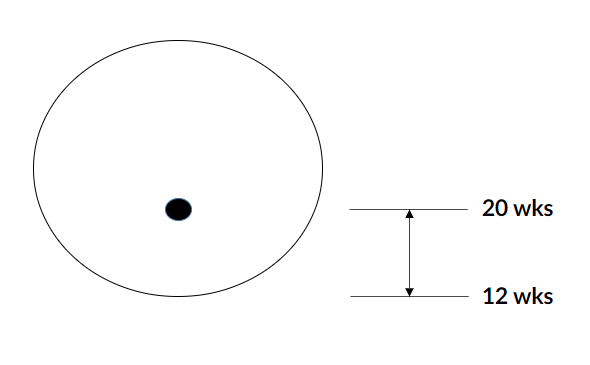
We have a crude diagram of this below where the dot represents the umbilicus. This would represent a fundal height that is consistent with 20 weeks gestation.
The base of this diagram represents the pubic synthesis. This would represent a fundal height that is consistent with 12 weeks gestation.
©2019 BoardsMD
Fundal Height
If we have the fundal height, measured in centimeters, then this should be equivalent to the gestational age in weeks.
This is particularly true after 20 weeks where this is most commonly used as an actual measure and as part of the standard physical exam when we are monitoring our pregnant patients.
It should be noted however that this is an imperfect and imprecise measurement with a precision that is plus or minus three weeks.
Fundal height while a favorite on question stems and for the purposes of examinations is not really all that useful clinically as we will see moving forward.
Therefore, we will need more invasive testing.
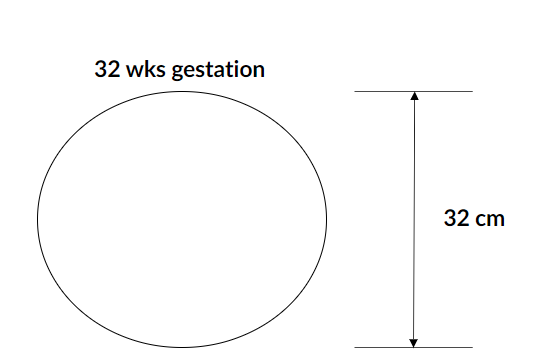
We have an example below of a pregnant woman's belly.
©2019 BoardsMD
The fundal height here has been measured at 32 centimeters, and this patient happens to be at 32 weeks gestation.
Therefore, we can say that the fundal height is appropriate for this patient's gestational age.
Short Fundal Height
There are instances where the fundal height is not consistent with the patient's gestational age. for example, in the case of a short fundal height.
In the case of a short fundal height, what we have is a case in which the fundal height is less than the gestational age.
The most common cause of this discrepancy of a short fundal height is actually inaccurate dates.
However, there are some other very high yield causes, including:
- Oligohydramnios,
- being small for gestational age
- having Intrauterine Growth Restriction (IUGR).
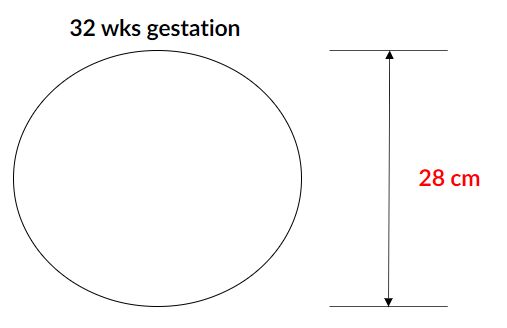
Below we have a patient who is 32 weeks gestation. However, their fundal height is only 28 centimeters.
©2019 BoardsMD
This is consistent with a short fundal height and therefore on examination questions, we can use this to narrow down our answer choices and to keep in mind these important causes:
- inaccurate dates,
- Oligohydramnios,
- being small for gestational age
- intrauterine growth restriction (IUGR).
Large Fundal Height
Just as we can have a patient who has a short fundal height, we can also have a patient who has a large fundal height.
In this case, the fundal height as measured in centimeters will be greater than the gestational age as measured in number of weeks.
This has several important high yield causes as well, including:
- Multiple gestation
- Molar pregnancy
- Polyhydramnios
- Large for gestational age
- Gestational diabetes or an increase in maternal weight throughout the pregnancy
- Placental abruption and
- Fibroids
When you think about these various causes, we can really think of all of them as adding additional mass or fluid essentially to the pregnant woman's belly.
For example, if we have multiple gestation or an increase in the amniotic fluid, or we have fibroids that are essentially bulging out of the uterus. Then it would be expected that the fundal height may be increased relative to the patient's gestational age.
There is simply more mass or more fluid that is causing this discordance.
We have an example of this below, where we have this crude representation of a patient's belly.
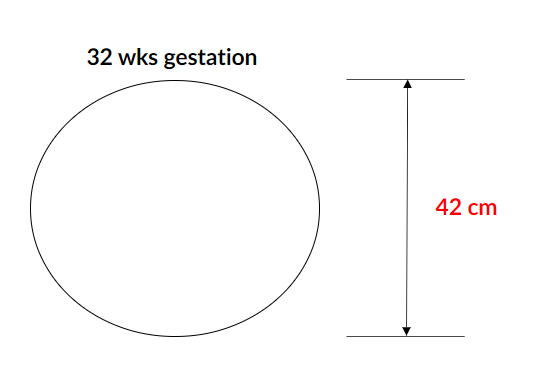
©2019 BoardsMD
This particular patient happens to be at 32 weeks gestation. However, her fundal height is discordantly large compared to this at 42 centimeters.
This would be referred to as a large fundal height at which point, we could look at these various causes as being the source or the route or the etiology of this finding.
Keep this in mind as It helps significantly in narrowing down your answer choices on examination questions.
Antepartum Fetal Surveillance
When it comes to antepartum fetal surveillance, the goal in using the various modalities that support this are to evaluate fetal well-being. Depending on the well-being of the fetus, as evaluated and determined by these various modalities, the management thereafter can become quite nuanced.
We will go through the management steps for using each of these tools in detail. When we refer to fetal surveillance, we are really referring to the tools, gadgets, and tests that we use to evaluate the well-being of the fetus.
These include:
- Non-Stress Test (NST)
- Contraction Stress Test (CST)
- Biophysical Profile (BPP)
- Umbilical Artery Doppler
On examination questions, you may need to determine whether fetal surveillance is going to be indicated at a given point in time in a given patient scenario. At the medical student level, there are really just three key scenarios that you need to commit to memory:
- A decrease in Fetal movement may raise concerns about the status of the fetus and its wellbeing.
- Being at least 41 weeks gestation. hen the fetus gets to this gestational age, there is an increased risk of complications and therefore there is need to keep a closer eye on the fetus with the use of our various tools.
- Being at, at least 32 weeks gestation in an at-risk pregnancy
Scenarios that place patients in an at- risk pregnancy category:
- Diabetes (including Gestational Diabetes)
- Hypertension (including Gestational Hypertension)
- Hyperthyroidism
- Intrauterine Growth Restriction (IUGR)
- Systemic Lupus Erythematosus (SLE including Antiphospholipid Syndrome)
- Oligohydramnios
- Isoimmunization
- History of fetal demise
- Sickle cell disease
Non-Stress Test (NST)
One of the major outputs of the NST is the fetal heart rate tracing. There are several fetal heart rate tracings that you should be aware of and know how to interpret in the context of examinations:
- Accelerations
- Early decelerations
- Late decelerations
- Variable decelerations
- Sinusoidal pattern
Our page on fetal heart rating tracings goes into specifics on each of these.

©2019 BoardsMD
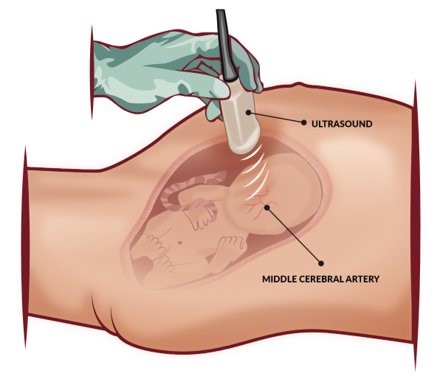
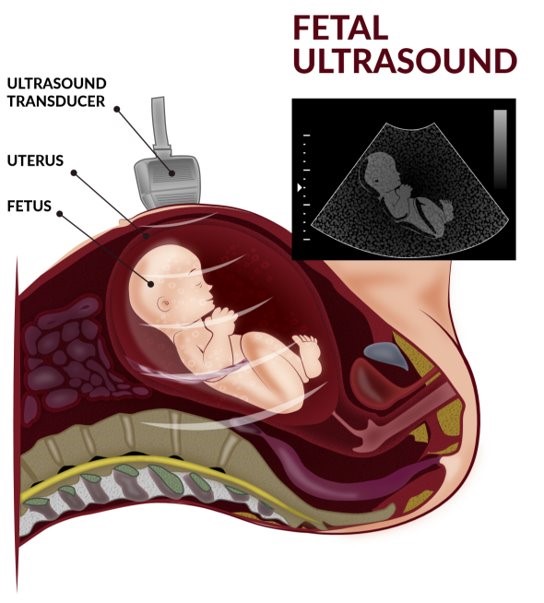
As shown in the image above, in an NST there is:
- A transducer which senses the uterine contractions.
- A transducer which senses the fetal heart rate, thus generating a fetal heart tracing which allows us to assess the status of the fetus.
Terminologies of NST and the values of interest
- Baseline: 110-160 beats per minute
- If the baseline is greater than 160 bpm, then the fetus is said to have fetal tachycardia.
- If the baseline is less than 110 bpm, then the fetus is said to have fetal bradycardia.
- Variability: This is a measure of how much the baseline undulates as we move along the fetal heart rate tracing.
- The NST has moderate variability if it is between 6 and 25 bpm in terms of variation around the fetal heart rate baseline.
- Accelerations: Increases in the fetal heart rate.
- These are said to be reassuring on a fetal heart rate tracing if there are at, at least 2 heart rate increases, which are at least 15 bpm, and last for at least 15 seconds within a 20-minute period.
- Decrease in the fetal heart rate. These include:
- Late decelerations
- Early decelerations
- Variable decelerations
©2019 BoardsMD
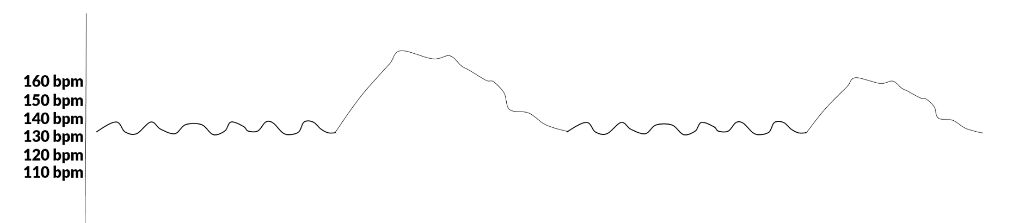
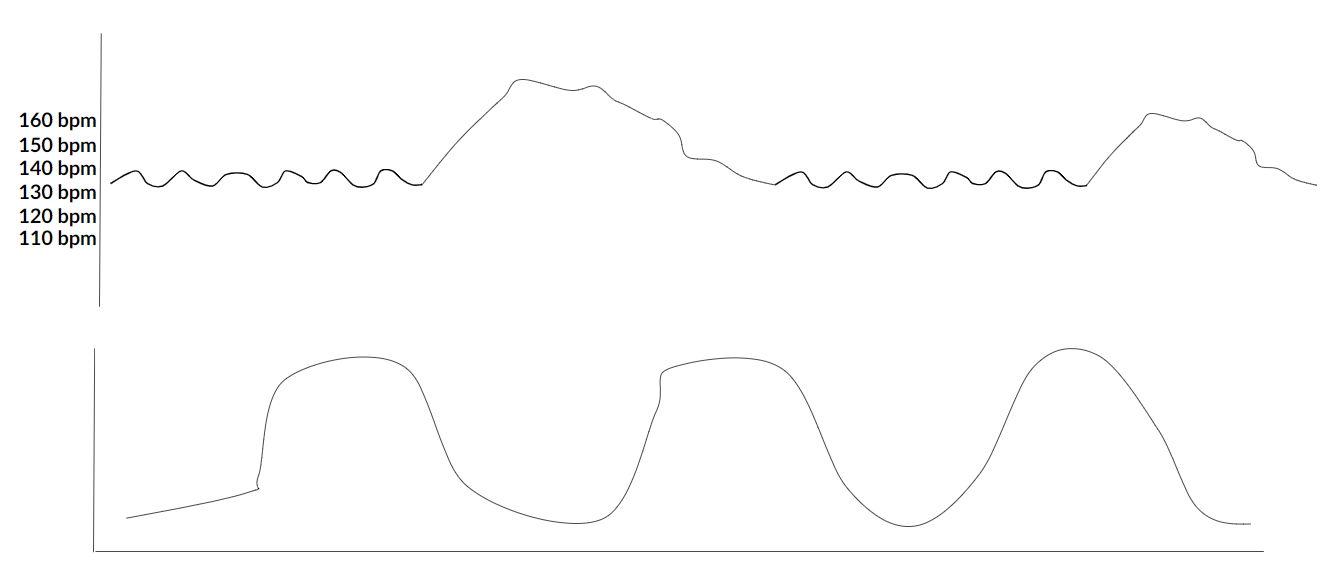
An example of a heart rate tracing that has been generated from a Non-stress Test.
- Baseline: Approximately 135 bpm. This is considered a normal fetal heart rate.
- Variability: The undulations about the baseline, in which it is considered moderate because they are between 6 and 25.
- There are no decelerations in this case.
- There are two accelerations that are at least 15 bpm each for at least 15 seconds each. This said to be a reassuring NST and that there is no evidence here of significant fetal distress.
Nonreactive NST
Presentation
In the case of question vignettes this will present with one of the 3 major indications of NST:
- Decrease in fetal movement
- At-risk pregnancy in which case NSTs will begin at 32 weeks gestation
- Normal pregnancy in which case we are post term and having an NST at 41 weeks.
Pathophysiology
The 2 major causes are either:
- The baby is sleeping in which case it is not going to be reactive
Or
- There is fetal distress and fetal hypoxia.
Wikicommons - Woodley Wonderworks
Diagnosis
- Less than 2 accelerations within a 20-minute period
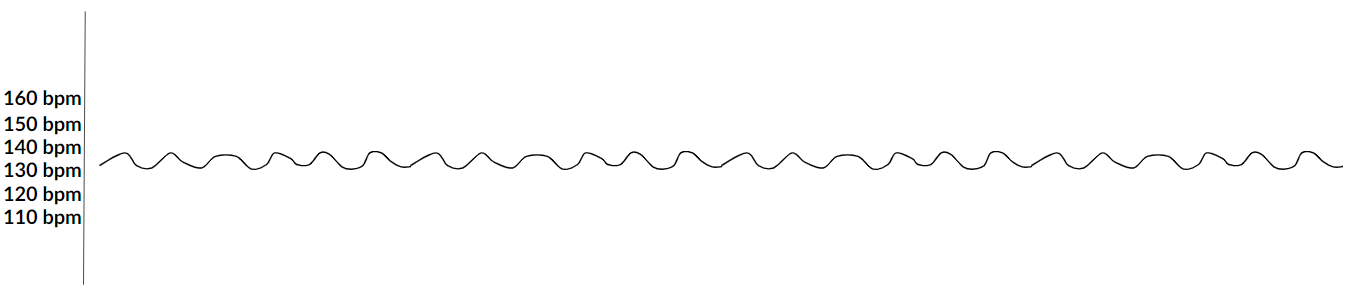
Example of a Nonreactive NST
- Baseline: About 135 bpm
- However, there are no accelerations. This is said to be a Nonreactive NST.
©2019 BoardsMD
Management
If the NST is nonreactive:
- Perform Vibroacoustic stimulation. This allows us to wake the fetus up, and if the ideology is that the fetus is asleep, this maneuver will allow us to wake the fetus up in order to ultimately get a reactive NST.
- Alternatively, we can extend the length of the NST for at least 40-60 minutes. This will allow the fetus to get up from its nap allowing us to get a reactive NST.
If the fetus is still having a nonreactive NST in spite of performing a Vibroacoustic stimulation or extending the NST for at least 40-60 minutes, proceed with:
- A contraction Stress Test (CST)
Or
- Biophysical profile
Summary
Indications for fetal surveillance:"
©2019 BoardsMD
As we stated previously, when we have a nonreactive NST we can either do a Contraction Stress Test or a Biophysical Profile.
Contraction Stress Test
In the case for a Contraction Stress Test, we have the key elements of a fetal heart rate tracing including;
- Baseline
- Variability
- Accelerations
- Decelerations
- Contractions. Which is considered to be normal if they add up to a total of at least 200 Montevideo units (MVU) in a 10 minute period. We discuss this in more detail in our lesson on fetal heart rate tracings.
CST Interpretation
When it comes to interpreting a CST, it's important to understand that we are inducing these contractions with either oxytocin administration or by stimulating the nipple of our female patients.
It's important to keep in mind here that we need to have at least three contractions in a 10 minute period in order to have what we consider an adequate CST.
What we are most concerned about in the case of having an abnormal or a positive test is to have late decelerations after at least 50% of the contractions. This is very concerning for field distress and will ultimately necessitate us to move towards delivery.
In the following chart, we have an example of a normal CST.
©2019 BoardsMD
As you can see at the bottom of the presentation, we have three contractions within a 10 minute period and therefore this is considered to be adequate in terms of nipple stimulation or oxytocin administration.
Additionally, we have the presence of two accelerations within this timeframe, and we see that there are no late decelerations or any other concerning features.
Therefore, this would be considered to be a normal or reassuring Contraction Stress Test.
Biophysical Profile (BPP)
After an abnormal NST that does not respond to vibroacoustic stimulation or waiting 40 to 60 minutes for the fetus to wake up, we can do a CST or we can perform a Biophysical Profile BPP.
©2019 BoardsMD
The BPP consists of five components, including an NST, as well as 4 ultrasound assessments.
Therefore, a BPP is a combination of NST and fetal ultrasound being used together in a scoring system to determine fetal wellbeing.
Overall, the five components are:
- NST - We should be able to see at least two accelerations in order to have a reassuring fetal heart rate tracing.
- Fetal Breathing - We are reassured if we can see at least one 30 second episode of rhythmic fetal breathing
- Fetal Movement - We want to be able to see at least three body or limb movements.
- Fetal Tone - We want to be able to see at least one instance of limb extension.
- Amniotic Fluid Volume (AFI) - The AFI is considered to be normal if it is greater than five centimeters. However, if the AFI is less than five centimeters then the fetus is said to have Oligohydramnios (low amniotic fluid). Another way to characterize the amniotic fluid volume that you may see in question stems is a measurement of the deepest vertical pocket on fetal ultrasound. The deepest vertical pocket is considered to be normal if it measures at least two centimeters in diameter.
BPP Score
The BPP score is going to be made up of 5 components including the NST and then 4 ultrasound components.
The BPP score is then going to be a sum of these different components with two points assigned for each component.
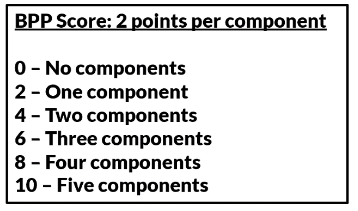
©2019 BoardsMD
Therefore, if we have no components present then the BPP score will be zero. This portends a very poor prognosis for the fetus.
This moves all the way up to having 5 of the components present with 2 points for each resulting in a BPP score of 10, which portends a very good prognosis for the fetus.
As we will see moving forward, this score is going to be essential in terms of determining the next step in management for the fetus.
BPP Score Management
- If we have a BPP score of 0 or 4, then this signifies that there is Uteroplacental dysfunction Therefore, if we see this BPP score in a board vignette, then our next step in management is induction of labor.
- If the BPP score is determined to be 6, then this is considered to be equivocal in which case we repeat the BPP in 24 hours.
- If the BPP score is 8 or 10, then this is considered to be normal and highly reassuring. In which case we repeat the BPP in one week, this is similar to what we saw previously, where if we have a reactive and reassuring NST, then we can simply repeat the NST on a weekly basis throughout the pregnancy.
- If we progress to the point of needing a BPP, we can simply repeat the BPP each week as long as it continues to be reassuring with high scores on this 0 to 10 BPP scoring system.
To summarize this scoring system and how it influences our management:
- If we perform a BPP and we have a score from 0 - 4, then we should proceed with induction of labor.
- If we have a BPP with a score of 6, then we should repeat the BPP in 24 hours.
- And lastly, if we have a reassuring BPP of 8 to 10, then we should repeat this test in one week.
Modified BPP (mBPP)
It is important to be aware of the fact that there is also what is referred to as a Modified BPP.
This has just two components which are the NST and the Amniotic Fluid Volume, which is extremely important in terms of determining the presence of amniotic fluid.
In this binary scoring system of the modified BPP, we first look at the NST and we are reassured if we can see at least two accelerations.
Then similar to our full-fledged BPP, we look at the amniotic fluid volume where we ultimately look to see that there is an AFI greater than five in which case we are reassured that we are not dealing with oligohydramnios (low amniotic fluid).
In question stems, you may also see this as having the deepest vertical pocket being at least two centimeters in diameter.
With the mBPP rather than having this 0 to 10 scoring system, we really are dealing with a binary system where if we have both of these features being reassuring, then we have a normal mBPP.
If one or more of these features is not reassuring, we consider the mBPP to be abnormal at which point the next step in management is to proceed with induction of labor.
CST vs BPP
If on an examination question, you have a situation where you have a nonreactive NST and you must decide between a CST and a BPP, you should choose a BPP.
This is because the CST does have some relative contraindications given the fact that you are essentially inducing contractions with the use of oxytocin or nipple stimulation.
These relative Contra indications for the CSTs include
- High risk of preterm labor
- Preterm Premature Rapture of Membranes (PPROM)
- History of a Syrian delivery or myomectomy
- Placenta previa.
In contrast, the BPP has no indications.
Therefore, if faced with a decision between these two modalities, you should go with the BPP especially in a patient who has one of these relative Contra-indications.
Umbilical Artery Doppler
The major indication for the use of an Umbilical Artery Doppler is Intrauterine Growth Restriction (IUGR). This is defined as having a size for gestational age, which is less than the 10th percentile.
If we were to perform an Umbilical Artery Doppler on a normal fetus, we would see High-velocity diastolic flow.
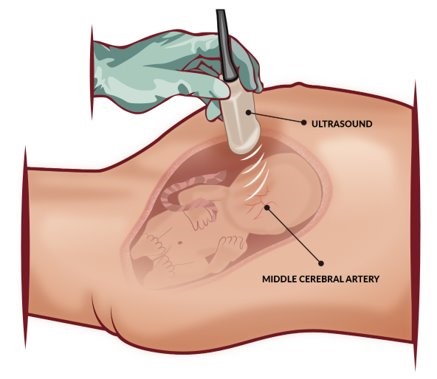
©2019 BoardsMD
In contrast, an Umbilical Artery Doppler is considered to be abnormal if we have absent or even reverse diastolic flow.
So, if an Umbilical Artery Doppler performed and we see absent or reverse diastolic flow, this is considered to be abnormal in this fetus is considered to be at high risk.
Approach to Fetal Surveillance
If we have decreased fetal movement, a pregnancy that is post-term, or an at-risk pregnancy at at least 32 weeks gestation, then we should proceed with an NST.
If the NST is non-reactive, we have the choices of vibroacoustic stimulation or extending the NST at which point if it is still non-reactive we proceed with a CST or BPP.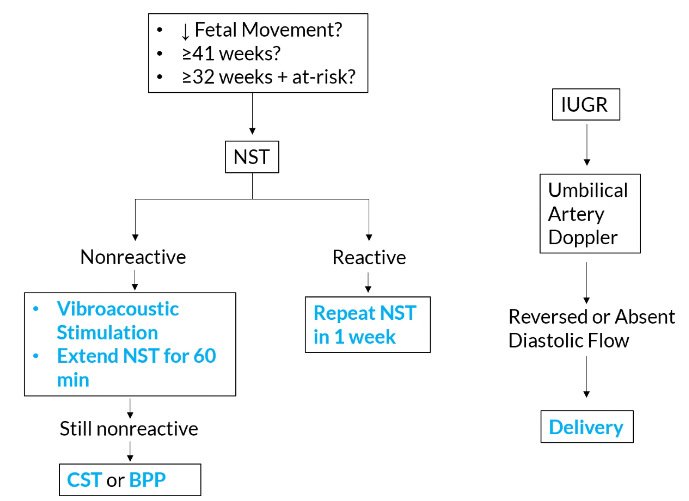
©2019 BoardsMD
If the NST is reactive, we simply repeat it in one week.
If we have a fetus with Intrauterine Growth Restriction (IUGR), we can perform an Umbilical Artery Doppler.
If an Umbilical Artery Doppler shows reversed or absent diastolic flow, then we should proceed with delivery
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
