Fetal Heart Rate Tracings
In This Module:
- Five Key Components of Fetal Heart Rate Tracings
- Early Deceleration
- Late Deceleration
- Variable Deceleration
- Oligohydramnios
- Fetal Tachycardia
- Sinusoidal Pattern
- Approach to FHR Training
In this section, we'll review fetal heart rating tracings. Before we delve into some of the high-yield pathologies in this topic, we'll first review some of the key components that go into these tracings.

©2019 BoardsMD
Pictured here is a typical schematic of a fetal heart rate tracing. We can see the actual fetal heart rate represented here in beats per minute or BPM on the top half of this schematic.
The fetal heart rate will oscillate up and down, up and down. By interpreting changes in the fetal heart rate over time, you can use these tracings to help us measure the health and viability of the fetus and to determine whether any intervention is required.
On the bottom half of this schematic, we have the contractions coming from the mother. The strength of these contractions are measured by a device called a tocometer which quantifies the strength of the mother's contractions in terms of Montevideo units (MVU)
Five Key Components of Fetal Heart Rate Tracings
In order to fully understand and interpret these fetal heart rate tracings, there are five key components that we must be able to understand and apply:
- Baseline
- Variability
- Accelerations
- Decelerations
- Contractions
Baseline
The first of these components is the baseline which refers to the fetus’s baseline heart rate.
A normal fetal heart rate baseline is defined as being 110 to 160 beats per minute. Therefore, if we are higher than 160 beats per minute, then we have a case of fetal tachycardia.
If our baseline is less than 110 beats per minute, then we have a case of fetal bradycardia.
Looking back at our sample of fetal heart rate tracing, we can see that the fetal heart rate is undulating back and forth with the central point or baseline of these undulations being right around 135 beats per minute.
Because this baseline fetal heart rate falls between 110 and 160 beats per minute, we can safely say that this fetus has a normal fetal heart rate and is not currently experiencing fetal tachycardia or fetal bradycardia.
Variability
The second essential key component is variability, which is the extent to which the fetal heart rate undulates around the given baseline.
In a fetal heart rate tracing the variability will be moderate, which occurs when there is a variability of 6 to 25 beats per minute.
Other possible categories of variability, which are considered to be abnormal, include minimal variability, where the variation around the baseline is less than or equal to five beats per minute.
We can have marked variability where the variation is greater than 25 beats per minute.
Or we can have absent variability where the variability is actually undetectable.
If we take a look back at our fetal heart rate tracing here, you can see that around our baseline of 135, we can see this undulation back and forth and the variation about the baseline goes between approximately 130 and 140 beats per minute.
Therefore, we would say that this fetal heart rate tracing has moderate variability as this variability of 10 beats per minute falls between our parameters of 6 to 25 beats per minute. In order to qualify as moderate variability.
Accelerations
The third key component is accelerations, which are defined as increases in the fetal heart rate. We consider a fetal heart rate tracing to be reassuring if there are at least 2 of these heart rate increases with an increase of at least 15 beats per minute.
In addition, these heart rate increases must last at least 15 seconds and occur within a 20-minute period.
We have here a sample fetal heart rate tracing and we can clearly see here that there are these 2 instances of an increase in the fetal heart rate.

©2019 BoardsMD
Now we must take note here and be sure that these increases are at least 15 beats per minute, and that they last for at least 15 seconds each
Because this fetal heart rate tracing appears to meet these criteria in terms of these accelerations, we would state that at least in terms of the accelerations, this fetal heart rate tracing is reassuring.
Decelerations
The fourth key component or the Decelerations, which are decreases in the fetal heart rate.
These decelerations come in three different types, including early, variable and late decelerations.
By the end of this lesson, you will be an absolute master when it comes to answering questions regarding both the diagnosis and management of these three deceleration types.
Contractions
The fifth and final component of fetal heart rate tracing is contractions.
Contractions are considered to be normal if there is a total of at least 200 Montevideo units within a 10 minute period of time.
In order to add up the Montevideo units (MVUs) for a given set of contractions, we should assess the size of each contraction individually. We do this by starting at the lowest point of the contraction, which in the case of the leftmost contraction in the image below begins at 10 MVUs
©2019 BoardsMD
We then identify the highest point of this contraction, which is at 100 MVUs.
We then subtract the highest point, which is 100 in this case, from the lowest point, which is 10 in this case
Doing some basic subtraction here, we can see that 100 minus 10 will give us 90 MVUs for this particular contraction.
If we then apply this same procedure to the other two contractions, we can see that each of these three contractions has a contraction strength of 90 MVUs.
So, if we simply multiplied this number 90 by 3, we will get 270 MVUs as our total over this 10 minute period
Because 270 is greater than our cutoff of 200 MVUs, we can say with confidence that the contractions in this fetal heart rate tracing are of adequate strength.
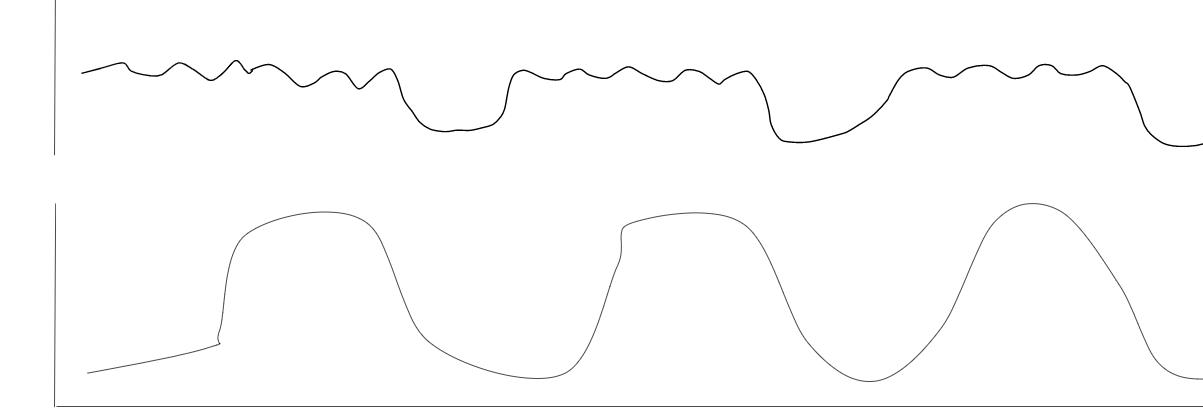
Early Deceleration
In early deceleration, our patient is going to be a mother in labor who presents with the following fetal heart tracing.

©2019 BoardsMD
On the bottom half of our tracing, you can see these contractions. On the upper half of the schematic, you could see these decelerations or drops in the fetal heart rate before returning back to this baseline.
Characteristically in an early deceleration, the deceleration is occurring just as the contraction is also beginning such that the lowest point or nadir of the fetal heart rate dropping is lined up with the highest point or peak of the contraction.
Pathophysiology
The pathophysiology of an early deceleration is compression of the fetal head.
This is not particularly alarming because there are many reasons that the fetal head can be compressed, especially as the fetal head becomes engaged during labor.
This compression of the fetal head ultimately leads to increase activation of the vagus nerve. Because we have increased vagus nerve activation and increased vagal tone, this will ultimately cause a decrease in the fetal heart rate, thus resulting in early deceleration.
Diagnosis
We simply look at the fetal heart rate tracing. The lowest point or nadir of the deceleration will be at the peak of the contraction.
We can once again see this in this early deceleration below where the nadir or lowest point of the deceleration in the fetal heart rate is lined up with the peak or highest point of the contraction.
©2019 BoardsMD
Management
And as we discussed previously, because this is simply a compression of the fetal head during a maternal contraction, it should be noted that no immediate intervention is needed and we can simply continue to monitor these patients.
Late Deceleration
Late Deceleration is also known as a late decel".
In a late deceleration, our typical patient is going to be a mother in labor who presents with the following fetal heart rate tracing;
As is evident in the name late deceleration, the deceleration will be late relative to the contraction such as the nadir or lowest point of the deceleration will occur after the contraction.
©2019 BoardsMD
Pathophysiology
The pathophysiology in the case of late decelerations is uteroplacental insufficiency, meaning that there is an insufficient supply of oxygen to the uterus and placenta relative to demand.
Some common scenarios where this uteroplacental insufficiency can occur include epidural injections. This is something that frequently shows up in question stems where the vignette will casually mention that the mother received an epidural and then they will show you a fetal heart rate tracing with the above characteristic pattern.
Other causes of uteroplacental insufficiency include uterine hyperstimulation which may occur with the use of magnesium sulfate and various tocolytic agents.
Late decelerations can also occur as a result of uterine rupture.
Diagnosis
In diagnosing a late deceleration, it is once again worth noting that the nadir or lowest point of the deceleration will be after the peak or highest point of the contraction.
Unlike in our patients with early decelerations where no immediate management is required, in our patients with late decelerations, there are 3 key steps in management that we must follow in order to mitigate the uteroplacental insufficiency.
The first step is to place an oxygen mask. If there is uteroplacental insufficiency, there's insufficient delivery of oxygen to the uterus and the placenta.
Therefore, adding supplemental oxygen can be of use.
We must turn the mother onto her left side. In order to make sense of this let's review some basic anatomy recall from your anatomy studies.
The inferior vena cava or (IVC) is on the right side of the patient's abdomen. As the uterus grows during pregnancy, it can press upon the IVC which can potentially worsen blood flow to the uterus and placenta, thus promoting uteroplacental insufficiency and late decelerations.

Therefore, if we turn the patient onto her left side, this will displace the uterus off of the IVC, thus allowing maximal venous return and blood flow.
Lastly, we must also be sure to stop oxytocin. One of the potential underlying causes of late decelerations is uterine hyperstimulation.
So, if we have oxytocin or any tocolytics on board that may be causing stimulation of the uterus, then we should be sure to stop these agents until the late decelerations resolve.
Admittedly in clinical practice, these three steps will not always be performed, but for the purposes of examinations, we should absolutely follow these three key steps in management.
Variable Deceleration
Our patient is going to be a mother in labor with a characteristic fetal heart rate tracing.
When we say variable, what we mean is that the nadir or low point of the deceleration is in a variable location with respect to the contraction.

©2019 BoardsMD
The low point of the deceleration may be at the start of the contraction. It may occur between contractions.
It may occur at the end of a contraction, or it may occur after a contraction.
These variable decelerations are the result of umbilical cord compression. There are several high-yield causes of umbilical cord compression to be aware of these include:
- Nuchal Cord
- Umbilical Cord Prolapse,
- Oligohydramnios
Oligohydramnios
In oligohydramnios, the issue is that there's too little amniotic fluid.
Because there is an insufficient amount of amniotic fluid it is easy for the umbilical cord to become compressed as there is less amniotic fluid to protect it.
On examinations question, writers will typically present oligohydramnios with at least one of the following criteria.
The first of these potential criteria is having an amniotic fluid index (AFI) that is less than or equal to five
In order to determine the amniotic fluid index (AFI), the OB/GYN will take an ultrasound.
When interpreting the ultrasound, the OB/GYN will divide the uterus into four separate quadrants. Each of these quadrants will be assigned a number based on the amount of amniotic fluid in that particular quadrant.
When the values from each quadrant are added together and this number is less than or equal to five, then we have an AFI that is indicative of oligohydramnios.
The other way the question writers will tell you that the patient has oligohydramnios is by stating that the deepest vertical pocket is less than two centimeters on the ultrasound.
When we say vertical pocket, we are simply referring to collections of amniotic fluid in one of the four quadrants as shown in this ultrasound image here.

If we simply measure the deepest vertical pocket on the ultrasound across, and it is less than two centimeters on the ultrasound, then we are dealing with the case of oligohydramnios which once again is a major cause of variable decelerations.
Diagnosis
In order to diagnose a variable deceleration, we simply take a look at the fetal heart rate monitor, where we will see that the nadir or low point of the deceleration occurs at variable times.
Additionally, as highlighted here in red, these decelerations will often be in a V or w shape.
You can see several examples of this V or w shape in our fetal heart rate tracing below.
©2019 BoardsMD
Management
We treat these patients with an amnioinfusion, which involves injecting fluid into the amniotic cavity.
The idea here is that the umbilical cord is being compressed and in many cases, this is the result of insufficient amniotic fluid or oligohydramnios.
Therefore, if we perform an amnioinfusion and increase the amount of amniotic fluid, then this should provide additional protection for the umbilical cord, thus relieving the umbilical cord compression and resolving the variable decelerations.
Fetal Tachycardia
In fetal tachycardia, our patient is going to be a mother in labor with a characteristic fetal heart rate tracing.
Specifically, the fetus will have a heart rate that is greater than the upper end of normal, which when it comes to the fetal heart rate baseline is 160 beats per minute.
Pathophysiology
The pathophysiology of fetal tachycardia is maternal fever and there are several potential causes of this, including:
- Chorioamnionitis
- Maternal hyperthyroidism
- Placental abruption, which we have an image of below
- Tocolytics

Diagnosis
In order to diagnose fetal tachycardia, we take a look at the fetal heart rate baseline and see that it is at least 160 beats per minute.
We can see this clearly in the fetal heart rate tracing below, where we could see that the baseline is roughly around 185 beats per minute which exceeds our normal range of 110 beats per minute to 160 beats per minute.

Management
The management of fetal tachycardia depends entirely on the etiology.
If we are dealing with a case of chorioamnionitis, then we will treat these patients with broad-spectrum antibiotic coverage, such as clindamycin with gentamycin.
If the fetal tachycardia is a result of maternal hyperthyroidism, then we can treat these patients with Methimazole.
If the patient has a placental abruption, particularly if she has significant fetal distress, then the definitive management for these patients is a cesarean delivery.
Sinusoidal Pattern
In a sinusoidal pattern, our patient once again is going to be a mother in labor, or she may present for routine screening or a regular antepartum visit, particularly in a mother who has anti-D antibodies.
The development of hydrops, in this case, is relevant because the underlying pathophysiology of the sinusoidal pattern is fetal anemia. This is an extremely high yield principle to be aware of.
The key to identifying a sinusoidal pattern is to recognize that the fetal heart rate tracing will go up and down, up and down in an undulating fashion.

©2019 BoardsMD
However, when you look closely at the tracing, you'll note that there is no variability or little variations throughout the tracing. Rather there is simply this consistent undulation and this lack of variability is highly characteristic of a sinusoidal pattern.
Diagnosis
In terms of diagnosis, the fetal heart rate tracing will show a sinusoidal pattern that will reveal no variability.
If we perform a Middle Cerebral Artery (MCA) Doppler, we will have an increase in the peak systolic velocity. This simply tells us that the blood is flowing more quickly in order to make up for the fetal anemia and to be able to deliver sufficient oxygen and nutrients to the fetal tissues.
This is something that we discuss in more detail in our lesson on fetal surveillance.
When we perform a fetal ultrasound, those with a sinusoidal pattern will have a pleural/pericardial effusion, as well as scalp edema.
Although this may be difficult to appreciate at the med student level, if you look at the bottom left corner of the picture below, this is depicting the thorax of the fetus with this structure here, being the fetal heart. Normally there would not be fluid surrounding this heart.
However, we can clearly see that there is this additional fluid represented by this black space that is collecting around the heart.

This just so happens to be a pericardial effusion, but just keep in mind that if you see any additional collecting of fluid, such as ascites, pleural/pericardial effusions, or scalp edema, then this may be yet another clue that we are dealing with a sinusoidal pattern.
Management
The management of these patients both depends on the number of weeks of gestation, as well as the severity of the anemia.
If we have a severe anemia prior to 32 weeks gestation, then the next step in management is to administer a Fetal RBC transfusion. This will allow us to treat the anemia in the meantime so that we could wait until at least 32 weeks to deliver.
If there is a severe fetal anemia at 32 to 34 weeks gestation, then we should give corticosteroids in order to promote fetal lung maturity and subsequently deliver the baby.
If the fetal anemia is mild, then we can simply perform serial ultrasounds until a gestational age of 37 to 38 weeks at which point, we can consider delivery.
Approach to FHR Training
Throughout this article, we have covered the essentials of understanding fetal heart rate tracings, and I've reviewed some of the highest yield conditions that examiners like to use to test your knowledge of these tracings.
If you could take each fetal heart rate tracing and treat it methodically as if you were reading an EKG, for example, then be sure to go through the five key components, including the baseline, variability, accelerations, decelerations, and contractions.
If you simply keep these five key components in mind, then you should have no trouble at all in dominating these questions on your examinations.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
