Hypertension in Pregnancy
Table of Contents:
- Fetal surveillance Indications
- Short Fundal Height
- Chronic Hypertension
- Gestational Hypertension
- Preeclampsia without severe features
- Preeclampsia with severe features
- Eclampsia
- HELLP syndrome
- Approach to Hypertension in Pregnancy
Important principles for the purposes of examinations:
- Hypertension in pregnancy affect the way that we treat and manage our pregnant women. It matters significantly, and is therefore a frequently tested topic.
- Management of hypertension in pregnancy is different from those in our typical patients, especially because several of our usual antihypertensive agents are contraindicated due to their teratogenic effects.
Fetal surveillance Indications
As I stated earlier, hypertension in pregnancy has significant implications for management of our patients, in particular when it comes to fetal surveillance.

©2019 BoardsMD
Fetal surveillance includes the use of modalities such as:
- NON-STRESS TEST (NST)
- Contraction Stress Test
- Umbilical Doppler
Key indications for the use of the NST and our other fetal surveillance modalities include:
- Decreased fetal movement, as this indicates the potential that there has been an adverse event with the fetus.
- Being at or greater than 41 weeks gestation, as this is considered to be post term and therefore requires close follow up and monitoring.
Additionally, once we reach at least 32 weeks gestation, there are several conditions which will necessitate the use of fetal surveillance and closer follow up, which we will discuss in detail in other sections.
For our purposes here, I want to note that hypertension, including gestational hypertension, is on this list. And therefore, how we diagnose and treat hypertension in our pregnant patients matters significantly, both in clinical practice and on examinations.
Short Fundal Height
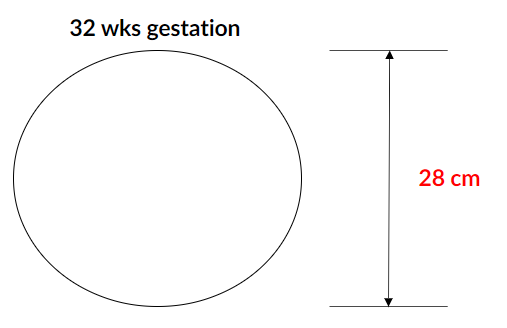
One classic situation in which you may see Hypertension suggested in a vignette is in the case of a short fundal height. A short fundal height is when the height of the fundus is less than we expect based on the gestational age.
Normally, in patient vignettes, when you have a fundal height, for example, of 28 centimeters, then you would expect for the gestational age to be equal to that number. In the image below, we would expect that the number of weeks gestation would be 28 weeks.
©2019 BoardsMD
However, as we can see in the image, the gestational age is 32 weeks, and therefore we can state that the fundal height is less than expected based on the gestational age.
The most common cause of this phenomenon is actually inaccurate dates as this can affect our ability to correlate the fundal height and the gestational age.
Other causes of short fundal height include:
- Being small for gestational age.
- Intrauterine Growth Restriction (IUGR).
Hypertension during pregnancy is a well-established risk factor for the development of Intrauterine Growth Restriction. Therefore, when you see a patient who has a short fundal height, although the most common cause is actually inaccurate dates, there are certainly scenarios in which the short fundal height is due to Hypertension.
The ultimately results in Intrauterine Growth Restriction, in particular Symmetric IUGR.
Special Considerations
Hypertension in pregnancy is DIFFERENT, especially in terms of how we manage the condition. Unfortunately, many of our typical antihypertensive medications are teratogenic.
This is especially true for ACE inhibitors and ARBs, which carry significant risks including the development of oligohydramnios, pulmonary hyperplasia and limb defects.
Therefore, when it comes to our Pregnant Patients, we really need to make sure that we stop these medications and substitute them with more appropriate antihypertensive therapy.
Chronic Hypertension
Presentation
Our classic patient is going to be an asymptomatic woman either prior to pregnancy or at less than 20 weeks of gestation.
Pathophysiology
The pathophysiology is an increase in total Peripheral Resistance amongst other factors.
Diagnosis
Blood pressure readings greater than 140/ 90 documented on two separate occasions. If necessary, we can use Ambulatory Blood Pressure Monitoring to achieve this.
Management
We use antihypertensive agents.

Antihypertensive Considerations
Since the antihypertensives that we typically use in our patients with elevated blood pressure are not as safe in our pregnant patients, we need to use specific antihypertensive agents.
These specific agents can be remembered by the mnemonic
Hypertensive Hydralazine
Moms α-Methyldopa
Love Labetalol
Nifedipine Nifedipine
On examination questions, the key in determining the correct antihypertensive for our particular pregnant patient is going to come down to choosing amongst the various side effects.
- Hydralazine: We should be concerned about potentially causing Drug-induced lupus in our patient.
- α-Methyldopa: While a well-studied and very safe antihypertensive in pregnancy, unfortunately only works in a long acting manner. Therefore, this is less appropriate for patients who need immediate reductions in blood pressure.
- Labetalol: This is, of course, a beta blocker and therefore we are concerned especially in our patients with Bradycardia.
- Nifedipine: A well-studied Calcium channel blocker, which can result in edema and dizziness.
Gestational Hypertension
Presentation
Unlike our patients with Chronic Hypertension, who can be pregnant women who are less than 20 weeks gestation, Gestational Hypertension will occur typically in an asymptomatic pregnant woman who is greater than 20 weeks gestation.
And I say asymptomatic because as we move into a symptomatic hypertensive patient, this is when we start to delve into Preeclampsia, Eclampsia and HELLP syndrome territory.
Pathophysiology
The pathophysiology of gestational hypertension is unclear and hotly debated.
Some experts believe that this may represent an early form of Preeclampsia. This is largely because having gestational hypertension in and of itself is actually inconsistent with the physiology of pregnancy.
In pregnant patients, the physiology of pregnancy actually results overall in a decrease in the Mean Arterial Pressure. Our pregnant patients have higher stroke volume and higher heart rate relative to non-pregnant patients, and this results in an increase in Cardiac Output in pregnancy.
The reality is that in pregnancy, there is a very significant decrease in the Total Peripheral Resistance. This is believed to be mediated via Progesterone Mediated Mechanism.
The overall result being that in pregnancy in general, the physiology moves our patients overall to having a lower blood pressure. However, Gestational Hypertension, as well as Preeclampsia, Eclampsia and HELLP syndrome are exceptions to this rule.
Diagnosis
- Patients will have a blood pressure reading that is greater than 140/90.
- They will have a normal UA.
And as we will see moving forward this normal UA will be extremely important in differentiating Gestational Hypertension from Preeclampsia.
However, please note that it is normal in pregnancy to have trace Proteinuria. We discussed this in more detail in our physiology of pregnancy articles.
Management
- It is important that we have close follow up first of all with a urinalysis in order to monitor for progression to Preeclampsia, in which we would see more significant Proteinuria likely 2+ or 3+ on urinalysis.
- In addition, as we stated previously in this article, Gestational Hypertension is an indication for fetal surveillance, which we often start with the use of a Non-Stress Test (NST).
Other than closely following our patients with this follow up urinalysis and NST, the management of Gestational Hypertension is much like our management of Chronic Hypertension in pregnant women, as we will once again manage these patients with the use of:
- Hydralazine
- α-Methyldopa
- Labetalol
- Nifedipine
Preeclampsia without Severe Features
Presentation
We shall have an asymptomatic pregnant woman at greater than 20 weeks gestation, who is going to present with:
- characteristic elevated blood pressure
- Findings on urinalysis, that we will address in a moment
Pathophysiology
Pathophysiology is believed to be abnormal placental development, especially of the placental arteries as well as arterial vasospasm.
Diagnosis
In order to have a diagnosis of preeclampsia without severe features, we're going to have:
- Blood pressure of at least 140/90
- At least one of the following in terms of urine protein:
- Urine dipstick that demonstrates +1 protein, and as we stated previously, trace proteinuria is normal in pregnancy, but once we reach +1 protein, we are now in the territory of preeclampsia, very high yield to keep that in mind.
- Protein creatinine ratio of at least 0.3.
- At least 300 mg of protein If we perform our gold standard 24-hour urine protein.
Management
Preeclampsia without severe features, and preeclampsia with severe features have different management.
For patients with preeclampsia, we're going to need close follow up with
- Urinalysis (UA) to monitor for further progression of the Preeclampsia
- Nonstress test (NST), because Preeclampsia being a form of Gestational Hypertension is an indication for fetal surveillance.
If our patient is at less than 37 weeks gestation, then we use our classic antihypertensive medications of pregnancy, which we can remember with the mnemonic Hypertensive Moms Love Nifedipine. These include:
- Hydralazine
- α-Methyldopa
- Labetalol
- Nifedipine
However, once a patient with Preeclampsia without Severe Features reaches 37 weeks gestation, then proceed with delivery.
This has been well documented in the research literature in that if we wait for these patients after 37 weeks, the rates of complications increase. Therefore, for a patient with preeclampsia without severe features we really should deliver at 37 weeks gestation.
Preeclampsia with Severe Features
Presentation
We are going to have a
Symptomatic pregnant woman who is greater than 20 weeks gestation. Classically, these patients will present with:
- Headache
- Visual Changes
- Right Upper Quadrant Pain (RUQ Pain)
Hence, we are now in the territory of preeclampsia with severe features.
Pathophysiology
The pathophysiology is going to be abnormal placental development, as well as arterial vasospasm.
Diagnosis
Because we are now in the territory of Preeclampsia with severe features, these patients are going to have:
- Higher blood pressures with systolic of greater than 160 and diastolic over 110 (160/110).
They must also have at least one of the following criteria, In terms of proteinuria, much like our patients with Preeclampsia without Severe Features:
- +1 protein on urine dipstick,
- A protein to creatinine ratio of at least 0.3, or
- At least 300 mg of protein in the urine on a 24-hour urine study.
Patients can also meet criteria for having severe features if they have:
- Platelets dropping below 100,000
- A creatinine of greater than 1.1
- An AST or ALT which is double their baseline value.
This is consistent with the right upper quadrant pain that we often see in these patients with severe features, pulmonary edema, as well as cerebral or visual symptoms.
Management
We are going to have close follow up with
- Urinalysis
- Nonstress Test (NST).
However, as I warned you previously, the management for our patients with severe features differs from our management of patients without severe features from 37 weeks for those who have preeclampsia without severe features to 34 weeks for those who have preeclampsia with severe features.
Just to flesh this out a bit further, if our patients are less than 34 weeks gestation, then we manage them with our typical antihypertensive agents of pregnancy, including:
- Hydralazine
- α-Methyldopa
- Labetalol
- Nifedipine
Additionally, once a patient with sreeclampsia with severe features hits 34 weeks of gestation, we should give these patients Magnesium Sulfate, which is essential as anti-seizure prophylaxis.
We should also plan on ultimately delivering these patients. Once we wait beyond 34 weeks in our patients with severe features, our risk of Eclampsia and the development of other complications, which may compromise both the mother and the infant, begin to increase.
Therefore at 34 weeks gestation, we really need to plan on delivery in our patients with Preeclampsia with Severe Features.
Indications
Magnesium Sulfate is:
- An essential medication as an Eclamptic seizure prophylactic agent
- A hallmark of management both in our patients with severe Preeclampsia as well as Eclampsia
- Essential in our patients with preterm labor at less than 32 weeks gestation.
This has several important functions including preventing the development of cerebral palsy in the newborn.
Toxicity
Because Magnesium Sulfate is such an essential agent in Obstetrics and Gynecology, we must also understand its toxicity.
- At lower levels of toxicity, Magnesium Sulfate can cause a decrease in Deep Tendon Reflexes (DTRs).
And in reality, all these toxicities of Magnesium Sulfate can be remembered if we simply keep in mind that
- Magnesium and Calcium are often exchanging with one another in opposite directions
As Magnesium moves into cells and Calcium moves out of cells, the ability of these cells to depolarize and fire off action potentials, and ultimately generate movement and muscle cells, begins to decrease.
This is responsible for:
- The decrease in deep tendon reflexes at lower levels of Magnesium toxicity
- The decrease in respiratory rate,
- The decrease in cardiac conduction
Management
Our first step of course, is going to be to stop Magnesium Sulfate.
Have supportive measures in place.
However, if patients do not respond to these measures, or have evidence of decreased cardiac conduction, and therefore evidence of severe Magnesium Sulfate toxicity then we should proceed with the administration of IV Calcium Gluconate. This really the ultimate antidote for Magnesium Sulfate toxicity.
It relies once again on the opposing relationship by which Magnesium and Calcium exchange with one another as they move into and out of cells.
Eclampsia
Presentation
Symptomatic pregnant woman at more than 20 weeks gestation with:
- Grand mal seizures
- Headache
- Visual changes
- Right Upper Quadrant Pain RUQ pain
Pathophysiology
- Abnormal placental development
- Arterial vasospasm
Diagnosis
Seizures are present
Management
- Look after Airway Breathing and Circulation (ABCs)
- Give the patient Magnesium Sulphate as seizure prophylaxis
- Use the appropriate antihypertensives of pregnancy:
- Hydralazine
- α-Methyldopa
- Labetalol
- Nifedipine
- Deliver the patient
- NB: in actual clinical practice this can get pretty nuance, but for purposes of examinations, once we have a patient with eclampsia, we really need to look toward how we are going to deliver the baby.
Once the baby is delivered, the symptoms should be resolved and the seizures should not typically last outside of the pregnancy.
HELLP Syndrome
Presentation
Last but certainly not least we have HELLP Syndrome which presents very similarly to patients who have preeclampsia with severe features, as well as eclampsia, in that the patient will be a symptomatic pregnant woman at more than 20 weeks gestation with:
- Headache
- Visual Changes
- Right Upper Quadrant pain (RUQ pain)
Pathophysiology
- Abnormal placental development
- Arterial vasospasm
Diagnosis
The key to differentiating HELLP Syndrome from other conditions such as Preeclampsia with Severe Symptoms is, in labs, the presence of at least 2 of the following:
- Hemolysis (Hemolytic Anemia)
- Elevated Liver Enzymes
- Low Platelets count
Question writers will some times only include two of the three criteria but that is indeed sufficient to get a diagnosis of HELLP Syndrome.
Management
HELLP Syndrome is really an indication for delivery. In patients at less than 34 weeks of gestation:
- Administer Corticosteroids in order to promote fetal lung maturity
- Administer Magnesium Sulfate in order to prevent the development of Cerebral Palsy in the newborn.
- Deliver the baby.
If the patient is at, at least 34 weeks gestation:
- Do not administer corticosteroids.
- Administer Magnesium Sulfate
- Deliver the baby
Other Liver Disorders of Pregnancy
While these disorders do not fit into our hypertension in pregnancy series, it is important to emphasize that there are some liver disorders that you should be aware of in addition to HELLP syndrome.
These include intrahepatic cholestasis of pregnancy, in which there is a very classic presentation of pruritis in the hands and feet, which isn't really present in any other condition.
We also have acute fatty liver of pregnancy, which classically presents with jaundice, hypoglycemia, and hypoammonemia, especially in the third trimester of pregnancy.
Once again, this combination of presentation isn't something you should expect to see in any other condition an examiner can throw at you.
Approach to Hypertension in Pregnancy
- Chronic Hypertension
- Gestational Hypertension
- Preeclampsia without Severe Features
- Preeclampsia with Severe Features
- Eclampsia
- HELLP Syndrome
Keep in mind:
- That these disorders starting from Gestational Hypertension all the way to HELLP Syndrome fall along a continuum in terms of severity.
- The key cutoffs in terms of the diagnosis as well as the differentials in management between these different conditions.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
