Physiologic Changes of Pregnancy
Table of Contents:
- Physiology of Pregnancy
- Blood Pressure
- Pearl: Benign Ejection Murmur
- Pearl: Peripheral Edema
- Renal Function
- Pearl: Protoeinuria
- UTI in Pregnancy
- ↑Minute Ventilation (VM)
- Pearl: Dyspnea of Pregnancy
- Dilutional Anemia of Pregnancy
- Hypercoagulable State
- GERD
- Constipation
- Pearl: Nausea and Vomiting
- Pearl: Hyperemesis Gravidarum
- Summary of Physiologic Changes of Pregnancy
High yield topic alert!
Physiology of Pregnancy
We will be covering several high yield physiologic changes that occur across various organ systems, including our cardiovascular system, renal, pulmonary, hematologic, and GI organ systems.
The key takeaway from this lesson is going to be that there are several changes during pregnancy (which will often be put in examination questions) that may seem abnormal. It may lead you to want to pursue additional diagnostic testing or look further into the patient's condition.
However, if we understand the physiology of pregnancy, then we can ultimately understand what is normal and therefore better understand what is abnormal as we move ahead.
Blood Pressure

One of the first things that we should know about pregnancy is that generally speaking, there should be a small decrease in the overall blood pressure of our patient.
This requires a bit of a deep dive into some of the individual values, which make up our blood pressure.
Recall from your physiology studies that the mean arterial pressure is equal to the cardiac output times the systemic vascular resistance.
MAP = CO x SVR
During pregnancy overall, there is going to be an increase in cardiac output. This is because there is an increase in the stroke volume and an increase in the heart rate.
Despite this increase in the cardiac output, which is ultimately going to go into our calculation of the mean arterial pressure, there is a massive decrease in the systemic vascular resistance which ultimately compensates for this increase in the cardiac output resulting in an overall decrease in the mean arterial pressure
This significant decrease in the systemic vascular resistance is a result of an increased level of progesterone during pregnancy which results in smooth muscle relaxation, ultimately resulting in a significant drop in our patient's systemic vascular resistance. Resulting in an overall drop in blood pressure during pregnancy.
Pearl: Benign Ejection Murmur
In addition to having lower overall blood pressures, another common finding that we may see in our pregnant patients is a benign murmur.
This is a result of increased intravascular volume resulting in increased blood flow, which essentially causes a flow murmur, which is completely benign.
Diagnosis
In, cardiac Auscultation we will hear it mid-systolic ejection murmur, which is best heard over the left sternal border.
Management
Because this represents a benign finding, we can simply perform routine follow-up in these patients.
However, if these patients have other symptoms which are concerning for vascular heart disease, or if they have a diastolic murmur on physical exam, then we should proceed with getting an echocardiogram in order to better evaluate for further cardiac structural disease.
Pearl: Peripheral Edema
In addition to lower overall blood pressure, as well as the presence of a benign systolic ejection flow murmur, another cardiovascular finding, which is normal in pregnancy is the presence of peripheral edema.
This is because as the gravid uterus continues to grow throughout the pregnancy, this will cause compression of the inferior vena cava (IVC)
This results in an increase in hydrostatic pressure, which forces fluid into the interstitium resulting in edema.
In the image below we have this uterus, which is expanding in size throughout the pregnancy.

This can ultimately compress on the inferior vena cava as this occurs, blood and fluid will pool in the lower extremities resulting in increased hydrostatic pressure and ultimately lower extremity edema.
Management
The first step in the management of a pregnant patient who presents with mild peripheral edema is simply to have that patient sleep on her left side.
This will displace the gravid uterus off of the IVC because the IVC is located more so on the right side of the body.
In the absence of any other underlying cardiac pathophysiology such as heart failure or cardiomyopathy, this simple maneuver of simply sleeping on the left side is going to help resolve this issue in the majority of our pregnant patients.
Don’t be fooled when you see the presence of peripheral edema on physical exam in a pregnant patient. This is an extremely common finding in pregnancy and often we do not need to go searching for intense or extremely concerning underlying causes.
Renal Function
One important finding that we will see very, very commonly in our pregnant patients is that they have an increase in urinary frequency.
There are several underlying physiologic changes that are responsible for this increase in urinary frequency.
The first of which is an increase in the size of the kidneys
Additionally, during pregnancy, there is an increase in progesterone, which results in smooth muscle relaxation, which causes an increase in both the GFR and the renal blood flow, as well as dilation of the ureter
With all of these changes going on, including larger kidneys accommodating more fluid and an increase in intravascular volume as well as increased renal blood flow, we are ultimately going to see an increase in the urinary frequency.
For pregnant patients who present with these symptoms, we should of course take their symptoms very seriously and should work them up appropriately with a urinalysis as well as a urinary culture.
Management
If this testing comes back normal, then for the majority of our patients with increased urinary frequency in pregnancy, we can simply reassure these patients and encourage them to continue hydrating.
It is extremely important to encourage this hydration in our pregnant patients because as we will see in some of our other lessons such as preterm labor, many patients will develop Braxton Hicks contractions as a result of dehydration in which they have cramps, which ultimately leads them to think that they are going into labor.
However, if we encourage our patients to continue hydrating and avoid having these cramps and Braxton Hicks contractions, then we can avoid putting our patients through the constant distress of recurrent visits to the emergency department thinking that they are going into labor when in reality, they are just dehydrated and cramping.
So even in the context of this increased urinary frequency, if we have a normal urine analysis, nothing comes back on the urine culture, the patient is otherwise asymptomatic, then we should really just reassure the patient and encourage them to do as they are currently doing in addition to continuing to hydrate.
Pearl: Proteinuria
Generally speaking for our non-pregnant patients, proteinuria is considered to be abnormal.
However, in our pregnant patients, it is important to understand that we give a little bit more leeway on this.
This is because in pregnant patients having trace protein on urinalysis or even 1+ protein is actually considered to be normal in pregnancy.
uring pregnancy, there is an increase in the GFR. This results in an increase in protein excretion. Therefore, we will lose some creatinine and some BUN in the urine, resulting in asymptomatic proteinuria.
Management
If we have a pregnant patient who is normotensive and happens to have trace protein on your analysis, then we simply resume normal follow-up with that patient, as this is considered to be a benign finding.
However, if the patient happens to have an increased blood pressure as well as trace protein, then we really need to evaluate that patient further for the presence of preeclampsia.
We discuss this in more detail in our lessons on hypertension in pregnancy.
For our purposes here, just know that having proteinuria plus an elevated blood pressure is definitely going to raise our suspicion for preeclampsia and eclampsia.
UTI in Pregnancy
In order to better understand the significance of UTI during pregnancy, we are going to do a brief review here of some of the physiologic changes that occur during pregnancy.
During normal pregnancy, there's overall an increase in progesterone levels.
These increased levels of progesterone ultimately act on the smooth muscle that surrounds the ureter. This causes the ureter to relax and ultimately expand and dilate.
Once this occurs, this makes it easier for bacteria in the bladder to ultimately ascend up the ureter and into the kidney resulting in pyelonephritis.
Because of this increased risk of pyelonephritis, we need to be much more careful in our pregnant patients when it comes to asymptomatic bacteria in the urine, as well as our less complicated UTI is due to this risk for progression to the involvement of the kidney.
Diagnosis
We are going to look at the urinalysis which will be positive, as well as the clinical picture including the presence or absence of CVA tenderness.
Management
If we have a case of asymptomatic bacteriuria or an uncomplicated UTI, then we treat these patients with Nitrofurantoin or amoxicillin.
Please note here that we are treating these cases of asymptomatic back to your area, as they have a risk of progression to pyelonephritis, as well as the potential to increase the risk of preterm labor in our pregnant patients.
In fact, eradicating this bacteriuria, urea is so essential that we actually have these patients return to the clinic in order to perform a test of cure, to make sure that we have eradicated the bacteria present in the urinary tract.
If our pregnant patient presents with fever or positive CVA tenderness, then we're more concerned about pyelonephritis. In which case we should admit the patient and ultimately give IV antibiotics, namely Ceftriaxone or Meropenem.
If after 48 to 72 hours, our pregnant patient is still symptomatic, then we should perform an ultrasound and ultimately may have to perform an incision and drainage. This is because the persistence of these symptoms raises our suspicion for the presence of an abscess.
In other clinical scenarios, you may see the use of a CT or an MRI in order to look for abscesses, but in the case of our pregnant patients, we will use an ultrasound instead as it poses less radiation risk and less potential for harm to the fetus.
Overall, the key takeaway from all of this management of UTI and pregnancy is that we take our asymptomatic bacteriuria extremely seriously, and that we ultimately may have to alter the way that we image these patients with suspicion, for abscess, vying for an ultrasound instead of a CT or MRI.
↑Minute Ventilation (VM)
During normal pregnancy, our pregnant patients are going to have an increase in their minute ventilation.
You will recall from physiology that minute ventilation is equal to the tidal volume times the respiratory rate.
During pregnancy, there's typically no change in the respiratory rate.
However, there is an increase in the tidal volume resulting in a subsequent increase in the minute ventilation.
As a result of this pregnant patients will typically present with a chronic respiratory alkalosis with metabolic compensation.
The key factor that causes this change in increase minute ventilation is once again, going to be an increase in progesterone levels.
This is because this progesterone stimulates respiratory centers in the medulla increasing the respiratory drive, increasing tidal volume and ultimately decreasing the patient's PCO2, which results in a chronic respiratory alkalosis.
Pearl: Dyspnea of Pregnancy
Another change in the respiratory system that we classically see during pregnancy is what we refer to as dyspnea of pregnancy.
This classically presents as a pregnant woman with shortness of breath.
However, there is no underlying pulmonary embolism or concerting etiology that we need to be concerned about.
This chronic shortness of breath has two key physiologic underpinnings; the first of which is an increase in progesterone, which stimulates the medulla, ultimately leading to an increase in the tidal volume but no change in the respiratory rate.
The second key physiologic factor in dyspnea of pregnancy is actually anatomic in nature. As the gravid uterus grows throughout the pregnancy, this is ultimately going to push up against the diaphragm, as the uterus begins to take up more and more room underneath the diaphragm. This causes the diaphragm to essentially push up against the lungs, which results in a decrease in the overall functional residual capacity or FRC.
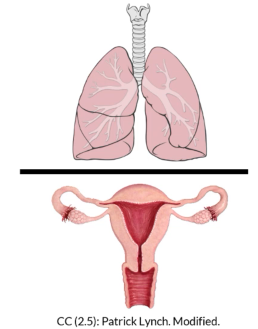
This decrease in the FRC ultimately leads to dyspnea or shortness of breath in our patients.
Dilutional Anemia of Pregnancy
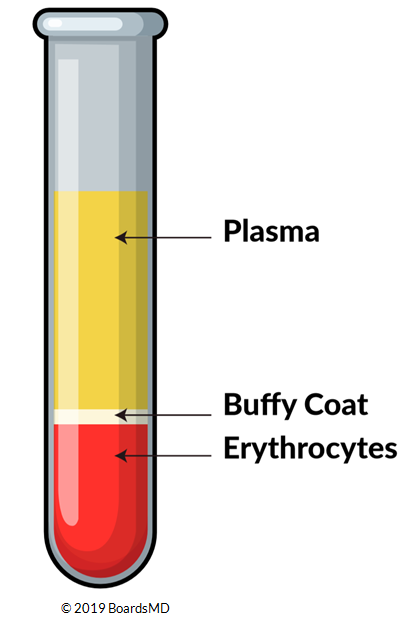
During pregnancy, pregnant patients will have an increase in erythrocyte production and therefore they will have an increase in their proportion of urethra sites.
However, they also have an increase in plasma, which is more significant than the increase in urethra sites.
By our hematocrit equation, we can see that if we have an increase in the number of red blood cells, but we have a disproportionately larger increase in the plasma, then overall, we will have a decrease in the hematocrit.
As a result of overall volume expansion and an increase in the plasma relative to the increase in red blood cells, our pregnant patients will typically have dilutional anemia at baseline.
As a result of this, our cutoffs for anemia during pregnancy are different from those in our typical healthy patients.
Hypercoagulable State
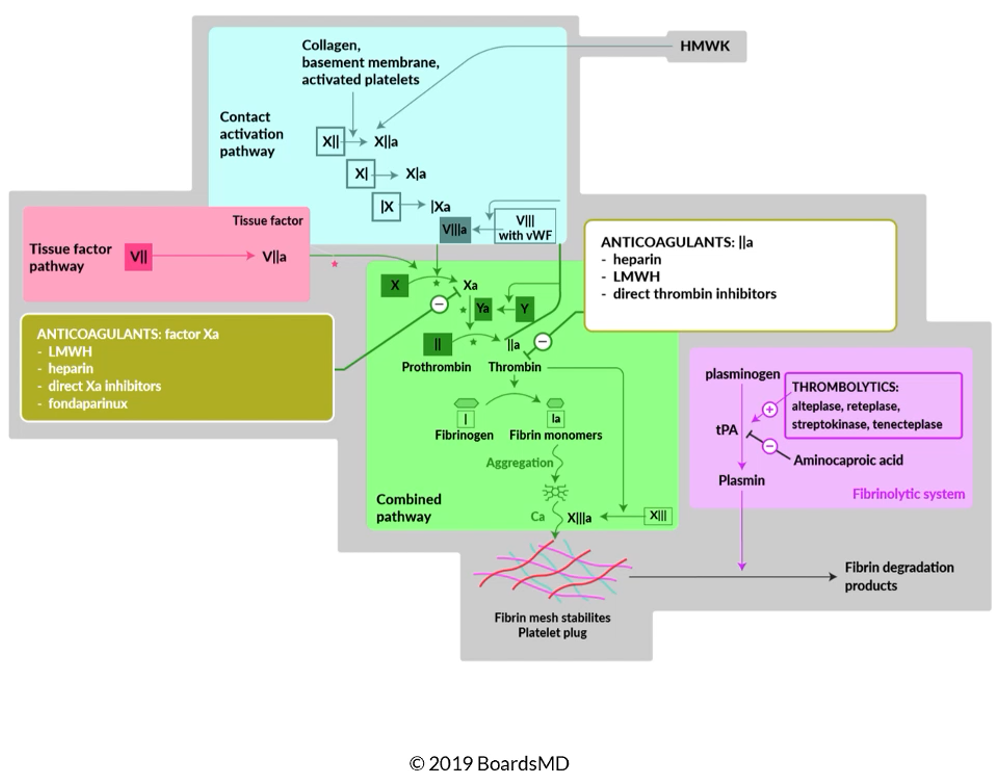
Another key physiologic change that we will see in the hematologic system, in our patients who are pregnant is that these patients will have a hypercoagulable state.
This is because, during pregnancy, there is an increase in Factor VII, VIII, IX, X as well as an increase in fibrinogen.
In addition to this increase in our coagulation factors, pregnant patients also have an increase in resistance to protein C as well as a decrease in protein S which further favors coagulability.
Therefore, it should make sense that during pregnancy or patients have an elevated risk of DVT and other complications related to their hypercoagulable state.
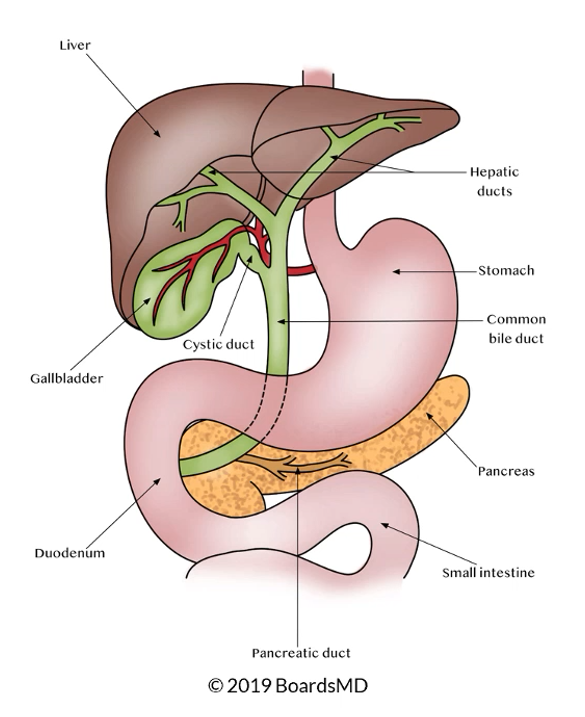
GERD
Our pregnant patients have an increased risk of developing Gastroesophageal Reflux Disease (GERD)
The underlying physiologic card because of this is going to be an increase in progesterone.
In particular, progesterone in this case causes relaxation of the lower esophageal sphincter, which allows additional acid to reflux from the stomach into the lower esophagus.
Management
These pregnant patients with GERD can be managed just like our usual patients with gastroesophageal reflux disease.
We can simply use a proton pump inhibitor, such as Omeprazole to control their symptoms.
Constipation
In addition to the development of GERD during pregnancy, it was also very common for our pregnant patients to have constipation.
This is a result of a decrease in gut motility, which results in these constipation symptoms.
Management
We can manage our pregnant patients with these symptoms by increasing fiber, as well as water intake and if necessary, we can use laxatives.
Overall, these symptoms of GERD and constipation are super common during pregnancy and occur in about a third of our pregnant patients.
Pearl: Nausea and Vomiting
There's also an increase in the incidence of nausea and vomiting during pregnancy, especially during early pregnancy.
This is believed to be due in part to the GERD that many of our pregnant patients develop, but it's also believed to be an effect of an increase in their levels of Beta-hCG.
Diagnosis
It is very important for us to be able to distinguish typical nausea and vomiting of early pregnancy for more serious conditions such as Hyperemesis Gravidarum.
The real key to this as we will see moving forward is that in normal nausea and vomiting of pregnancy, these patients will have no significant weight loss abnormalities.
This is in contrast to Hyperemesis Gravidarum where we can see significant changes in weight.
Management
In order to manage our patients with nausea and vomiting during pregnancy, we can:
- Modify their diet,
- Give them peradoxime as well as doxylamine. These both have strong evidence for efficacy during pregnancy.
- We can also give our patients Antiemetics such as on ondansetron.
Pearl: Hyperemesis Gravidarum
Patients with Hyperemesis Gravidarum will present with excessive vomiting, most common once again, in early pregnancy.
However, these patients will also have significant weight loss.
Etiology
The etiology of Hyperemesis Gravidarum is an increase in Beta-hCG. Risk factors for this include anything that will lead to a significant increase in Beta-hCG.levels. These include molar pregnancy as well as multiple gestations.
Below we have an example of a molar pregnancy with a classic snowstorm appearance on ultrasound.
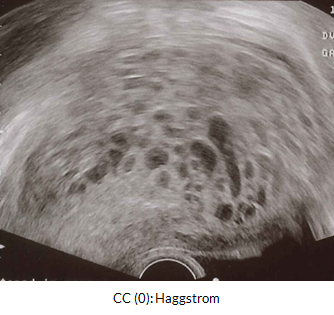
It should be noted that patients do not need to have a molar pregnancy or multiple gestations in order to develop this condition of Hyperemesis Gravidarum.
Diagnosis
In order to clinch the diagnosis of Hyperemesis Gravidarum, these patients will have at least a 5% decrease from their pre-pregnancy body weight. This represents a very drastic weight loss.
These patients may also present with unstable vital signs, including hypotension and tachycardia. These patients may also present with a metabolic alkalosis as well as a low urinary chloride as a result of their excessive vomiting.
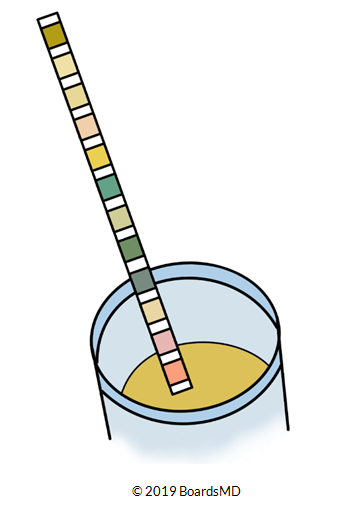
In addition, these patients also classically present with Ketones on urinalysis, so this is an important finding to look out for in our patients who were suspecting Hyperemesis Gravidarum.
The reason it is so important to distinguish Hyperemesis Gravidarum from normal nausea and vomiting of pregnancy is because the management in these patients is different.
Management
If our patient is suffering from Hyperemesis Gravidarum, we should ultimately admit that patient for the administration of IV Fluids, as well as IV Antiemetics until we have their condition under control.
If we do not take this seriously it can have serious consequences for both the mother and the fetus.
Generally, however, once we get out of the first trimester and later into the pregnancy, many patients with Hyperemesis Gravidarum decrease their symptoms. But sometimes we need to treat them inpatient to get them over that initial hump.
Summary of Physiologic Changes of Pregnancy
Cardiovascular changes during normal pregnancy include changes in blood pressure, the presence of systolic murmurs, as well as the presence of peripheral edema.
There is an increase in overall renal That it is normal to have trace proteinuria on your analysis during pregnancy and that pregnant patients have an increased risk for the development of UTIs.
During pregnancy, there is an increase in the minute ventilation, as well as chronic shortness of breath or dyspnea of pregnancy that many of our pregnant patients have.
Hematologic changes, including the dilutional anemia of pregnancy, as well as the fact that pregnancy in and of itself is a hypercoagulable state.
GI changes, which occur during pregnancy, including GERD, constipation, nausea, and vomiting, as well as the potential for the development of Hyperemesis Gravidarum.
The reason that the physiology of pregnancy is so useful as you navigate through exam questions is that once you know the normal of pregnancy, it becomes a lot easier to recognize what is abnormal and therefore what requires additional testing or intervention.
For example, if every time you see a pregnant patient and you overthink whether they have peripheral edema, benign systolic murmur on exam, trace proteinuria on their urinalysis, or a mild dilutional anemia, then you are going to end up chasing lab values and physical exam findings that are not going to help the patient or help you get the correct answer on the examination. And therein really lies the true value of this lesson’s series.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
