Maternal Infections
Contents
When studying maternal infections, take note that infections affecting the mother can ultimately affect the baby as well. We see this in a major way with genital ulcers, HSV, and other similar conditions.
There are several high yield maternal infections that we need to be aware of that can have significant effects on the fetus and ultimately the infant.
High yield topics in this section:
- UTI in Pregnancy can increase the risk of preterm delivery
- Group B Strep (GBS) can result in neonatal sepsis and understanding the management of GBS is essential, both clinically and on examinations.
- Chorioamnionitis can result in fetal tachycardia and fetal distress
- Maternal HIV, if transmitted to the newborn, can result in diarrhea and ultimately failure to thrive
This relationship between mother and fetus is going to be essential as we move forward.

UTI in Pregnancy
Presentation
When it comes to understanding UTI and pregnancy, we can break up UTI into three distinct categories.
The first of these categories is asymptomatic bacteriuria, in which the patient will have no symptoms, but will simply present with a positive urinalysis (+UA).
In contrast, in an Uncomplicated UTI, the patient may experience a +UA as well as be symptomatic, often with dysuria or increase urinary frequency.
Ultimately, these patients can progress to Pyelonephritis. These patients can additionally have a fever, nausea, vomiting, white blood cell casts on UA, as well as +CVA tenderness.
This tenderness of the costovertebral angle, as seen here in this image below is essential in distinguishing Pyelonephritis from less complicated UTIs.

Pathophysiology
In order to better understand the significance of UTIs during pregnancy, we're going to briefly review some of the physiologic changes that occur during pregnancy.
During normal pregnancy, there's overall an increase in progesterone levels. These increased levels of progesterone ultimately act on the smooth muscle that surrounds the ureter.
This causes the ureter to relax, and ultimately expand and dilate.
Once this occurs, it makes it easier for bacteria in the bladder to ultimately ascend up the ureter and into the kidney, resulting in pyelonephritis. Because of this increased risk of pyelonephritis, we need to be much more careful in our Pregnant Patients when it comes to asymptomatic bacteria in the urine, as well as our less complicated UTIs due to this risk for progression to the involvement of the kidney.
Diagnosis
When it comes to diagnosing a UTI, and pregnancy, we are going to look at the UA, which will be positive, as well as the clinical picture, including the presence or absence of CVA tenderness.
Management
If we have a case of asymptomatic bacteriuria or an uncomplicated UTI, then we treat these patients with nitrofurantoin or amoxicillin. Please note here that we are treating these cases of asymptomatic bacteriuria, as they have a risk of progression to pyelonephritis as as well as the potential to increase the risk of preterm labor in our regnant patients.
In fact, eradicating this bacteriuria is so essential that we actually have these patients returned to clinic in order to perform a test of cure to make sure that we have eradicated the bacteria present in the urinary tract.
If our pregnant patient presents with fever or positive CVA tenderness, then we are more concerned about pyelonephritis. In this case, we should admit the patient and ultimately give IV antibiotics namely Ceftriaxone or Meropenem.
If after 48 to 72 hours our pregnant patient is still symptomatic, then we should perform an ultrasound and ultimately may have to perform an incision and drainage. This is because the persistence of these symptoms raises our suspicion for the presence of an abscess.
In other clinical scenarios, you may see the use of a CT or an MRI in order to look for abscesses. But in the case of our Pregnant Patients, we will use an ultrasound instead, as opposes less radiation risk, and less potential for harm to the fetus.
Overall, the key takeaway from all of this management of UTI and pregnancy is that we take our asymptomatic bacteriuria extremely seriously and that we ultimately may have to alter the way that we image these patients with suspicion for abscess, vying for an ultrasound instead of a CT or MRI.
Group B Strep (GBS)
Presentation
This will typically be an asymptomatic patient who gets standard screening for GBS at 35-37 weeks.
Pathophysiology
The pathophysiology of GBS in the case of the pregnant woman is colonization of the vagina or rectum.
Diagnosis
This is going to be diagnosed with a rectal vaginal culture at 35 to 37 weeks. This is standard of care screening in all Pregnant Patients.
The reason for this being that GBS colonization in the mother poses a significant risk of the development of GBS bacteremia, and sepsis in the newborn.
Management
If the mother is found to have a positive screen, then we can administer penicillin G or Ampicillin during labor. However, if the patient has a penicillin allergy, we can ultimately give the patient clindermycin in order to treat and eradicate the GBS colonization.
Unknown GBS Status
Above we demonstrated the straightforward management of treating GBS colonization in a patient who clearly tests positive, however, the management becomes much more nuanced when it comes to an unknown GBS status of the mother. There are several potential criteria in the case of a mother with unknown GBS status that will cause us to treat the patient with antibiotics.
These include mothers who have unknown GBS status, but who have:
- maternal fever
- prolonged rupture of membranes
- preterm labor
- preterm premature rupture of membranes
- GBS bacteriuria during the current pregnancy at some point in time
- as well as a history of an infant with neonatal GBS
Having any of these characteristics is sufficient for us to go ahead and treat the patient with penicillin, as we are concerned about the infant potentially developing GBS, bacteremia, and sepsis.
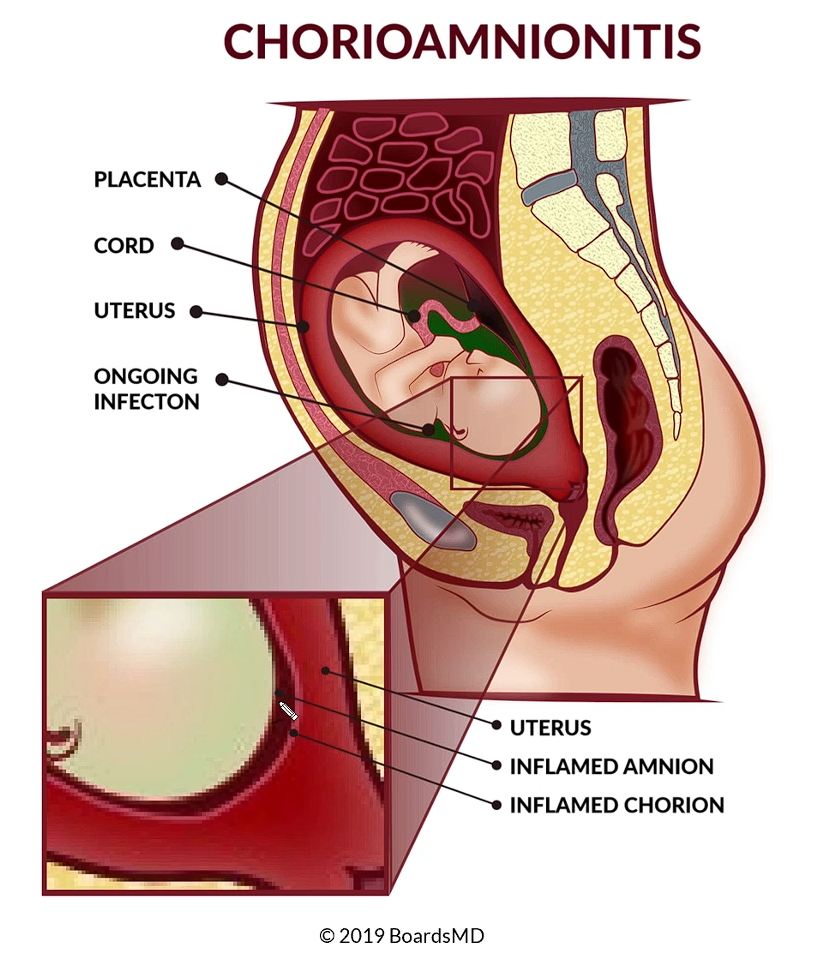
Chorioamnionitis
Presentation
This classically presents with maternal fever, uterine tenderness, and fetal tachycardia. This can be seen in the fetal heart rate tracing in the image below. Typically, a normal fetal heart rate is going to range from approximately 110 to approximately 160.
As we can see, on the y axis of this fetal heart rate tracing, this infant is hovering right around 185, or perhaps even 190 beats per minute, which is consistent with fetal tachycardia.

©2019 BoardsMD
Pathophysiology
The pathophysiology of chorioamnionitis is ascending vaginal flora, with Group B strep being the most common pathogen, once again, highlighting just how essential it is for us to screen with a rectal vaginal culture for all pregnant patients for the presence of GBS.
You can see below that we have a close up of the chorion in which we can see thickening and inflammation of the amnion as well as the chorion. Immediately adjacent to this, we have the foetus being subjected to this inflammation, as well as the elevated temperature, ultimately resulting in an increase in the foetal heart rate, as well as the development of fetal tachycardia in the context of chorioamnionitis.
Diagnosis
This is going to be a clinical diagnosis, as if we see the presence of maternal fever, fetal tachycardia, and uterine tenderness that we have the triad that is consistent with this condition. Rarely, if the diagnosis is unclear, we can perform an amniocentesis, which is considered the best test for Chorioamnionitis.
However, it is generally not going to be indicated.
Management
We will manage these patients with the use of broad spectrum antibiotics, a common regimen being Clindermycin/Ampicillin, plus Gentamicin. After the administration of antibiotics, if the fetal heart rate tracing is reassuring, then we can proceed with induction of labor and ultimately move towards a vaginal delivery.
However, if the tracing Nonreassuring that we should ultimately proceed with a Cesarian delivery so that the fetus is not further subjected to the infection and ongoing inflammation resulting from the chorioamnionitis
Maternal HIV
Presentation
The presentation of this is going to be dependent on the CD4+ count, and we discuss this in more detail in our infectious disease articles. It is important to note that HIV is going to be part of our universal screening at the first prenatal visit.
Pathophysiology
In terms of transmission of HIV to the fetus, this can occur as transplacental transmission or can occur during delivery. Therefore, our management is going to focus on making sure that this transmission does not occur between mother and fetus.
In terms of the mother's infection, this generally occurs via sexual contact or in some cases, needle stick, especially in the healthcare setting.
Diagnosis
The diagnosis of HIV is generally going to occur in pregnancy at the first prenatal visit with a measurement of the HIV viral load. After that point, it is standard of care for patients to get an HIV viral load, as well as a CD4+ count at least every 3 months from that point forward.
Management
The standard of care is Highly Active Antiretroviral Therapy (HAART). In HAART we use 2 Nucleoside reverse transcriptase inhibitors (2 NRTIs) plus one Protease Inhibitor.
Or instead of a protease inhibitor, we can also use a Non-Nucleoside Reverse Transcriptase Inhibitor (NNRTI). Among these agents it should be noted that Zidovudine actually has the best evidence.
Therefore, when deciding between different medications in the context of exam questions, you should favor Zidovudine if you were having to select between different medications that are part of the heart regimen.
Lastly, as one other important caveat in terms of the management of HIV and the context of delivery, if the patient is found to have a high viral HIV load that is greater than 1000, then we should proceed with Cesarian delivery in order to better protect the fetus and ultimately the infant from the transmission of this disease.
Neonatal HIV
The reason that we are so concerned about this transmission of HIV from the mother to the fetus, is that ultimately the infant can develop neonatal HIV. This classically presents with chronic diarrhea, recurrent infections due to the immunocompromised state of the infant, as well as failure to thrive.
This can be particularly devastating.
Wrapping Up
We have now covered some of the essential maternal infections when it comes to board examinations.
To Recap:
- UTI, which has completely different management in pregnancy relative to our typical patient.
- Group B Strep, which can ultimately result in bacteremia and sepsis of the newborn.
- Chorioamnionitis, which can cause significant fetal tachycardia and distress and
- HIV, which can ultimately result in failure to thrive of the newborn.
For more on the diagnosis and management of various maternal infections and how we manage these in the context of the fetus and ultimately the newborn, be sure to check out our article on Genital Ulcers in which we dive into these topics in detail.
Turn Crunch Time into Crush Time
We strive to make the most accessible and efficient boards exam study guide available. If you have any feedback, want us to add more info on specific topics, or would like to speak to us directly, please contact info@boardsmd.com.
Want to watch and listen on the go? Download the Kajabi app to access all of our study content, anywhere on your phone.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
