Postpartum Hemorrhage
In This Module:
- Defining Hemorrhage in Vaginal vs. Cesarean Delivery
- Lochia
- The Four T's
Defining Hemorrhage in Vaginal vs. Cesarean Delivery
Postpartum hemorrhage refers to blood loss during the postpartum period. Depending on whether there is a vaginal or cesarean delivery, the level of blood loss that is required to be classified as postpartum hemorrhage will be different.
In the case of a vaginal delivery if the blood loss exceeds 500 milliliters, then this is considered to be postpartum hemorrhage. Whereas in the case of cesarean delivery, blood loss greater than 1000 milliliters (1 liter) is considered to be postpartum hemorrhage.
When you are looking at question stems, always make sure to check whether there is a vaginal or cesarean delivery taking place before you read into the amount of blood loss to determine whether this is a postpartum hemorrhage question that you're dealing with.
Lochia
One trick that you may see on question stems in the context of post-partum hemorrhage is lochia which is a normal discharge that occurs from the vagina during the postpartum period.
Lochia Rubra
During the postpartum period, one to three days after delivery, we have lochia rubra, which is a normal discharge that tends to be red or red brown, and may even have clots in it.
Lochia Serosa
At three to four days postpartum, a patient may have lochia serosa which tends to be a pink or a pink Brown
Lochia Alba
At 14 to 21 days postpartum, a patient may have lochia alba, which tends to be a white or yellow discharge.
Identifying Lochia
All three of these types of lochia - lochia rubra, lochia serosa and lochia alba are completely normal in the postpartum period and do not qualify or concern us for postpartum hemorrhage.
It should be noted that the exact amount of blood may not always be given.
We may not have the value of 500 milliliters as is the cutoff for a vaginal deliveries or 1000 milliliters, which is the cutoff versus and deliveries.
If we see two blood-soaked pads per hour, then that is considered to be normal in terms of bleeding during the postpartum hemorrhage. However, if we exceed two blood-soaked pads per hour, then that is considered to be consistent with postpartum hemorrhage and excessive bleeding.
The Four T’s
As we attempt to organize postpartum hemorrhage in our mind, we can think of postpartum hemorrhage in terms of the Four T’s.
The Four T’s, stand for:
- Tone
- Trauma
- Tissue
- Thrombin
Tone: Uterine Atony
We will now dive into the first of the four T's, which is tone.
The first condition that we will discuss in this section is Uterine Atony, which is essentially a lack of uterine tone.
This occurs in a woman with a prolonged course of labor who develops postpartum hemorrhage.
© 2019 BoardsMD
Pathophysiology
The pathophysiology of uterine atony is insufficient myometrial contractions.
Normally in the postpartum period the placental arteries will begin to bleed.
When the myometrium contracts down on these placental arteries, this will cause the placental arteries to stop bleeding.
However, if the uterus is atonic, then bleeding from the placental arteries will continue and the patient will thus continue to hemorrhage.
Risk Factors
- Prolonged labor
- Oxytocin as a result of its tocolytic properties as this essentially tires out the uterus.
- Being large for gestational age (LGA)
- Multiple gestation
- Hypertension
- Use of Magnesium Sulfate,
- Chorioamnionitis
All of these are significant risk factors for the development of uterine atony, but prolonged labor and the use of oxytocin are by far the most common on examinations.
Diagnosis
Uterine Atony is largely going to be a clinical diagnosis.
This is going to be a patient who has postpartum hemorrhage, and also has an enlarged boggy uterus on physical exam.
Boggy uterus is a term that we only see in a handful of situations. These include Uterine Atony, Septic Abortion and Adenomyosis.
Therefore, if we have a boggy uterus in the postpartum period, especially in the context of postpartum hemorrhage, then we need to think about Uterine Atony.
Management
The management of uterine acne is extremely high yield.
- The first step in management is going to be uterine massage in order to give the uterus more tone so that we can clamp down on those placental arteries and stop the hemorrhage from occurring.
- If this is not sufficient, then we can give oxytocin once again to help that myometrium clamp down on the placental arteries.
- If the hemorrhage continues at this point, then we can give methylergonovine or Prostaglandin F2alpha (PGF2α). These agents do have some important side effects for us to be aware of. In the case of methylergonovine, it increases the patient's blood pressure. And in the case of Prostaglandin F2alpha (PGF2α), it can cause bronchospasm. Therefore, if our patient is hypertensive, then we will want to avoid methylergonovine, and if our patient has a history of asthma or COPD, then we will want to avoid Prostaglandin F2alpha (PGF2α). oftentimes the decision between these two medications is something you may need to be aware of for examination purposes.
If the hemorrhage still continues after these three steps, then we can proceed with a dilation and curettage (D&C).
If the hemorrhage is still occurring at that point, then we should proceed with a laparotomy as well as potentially a hysterectomy as at this point, we really have some serious life-threatening hemorrhage that is occurring.
In the schematic below, we show uterine massage, which is going to be the first step in management in the case of Uterine Atony.

As you can see here, we have one hand which is pushing down on the fundus from the exterior and we have the other hand coming in from the pelvic cavity and pushing up against the uterus from this direction.
The idea here, being that if we massage the uterus, then we can increase uterine tone and help that myometrium to really clamp down on the placental arteries thus stopping the hemorrhage.
Trauma
The first major cause of traumatic postpartum hemorrhage is going to be vaginal and cervical lacerations.
This will occur in the context of a forceps assisted or operative vaginal delivery in which there are instruments being used and we are manipulating the reproductive structures. This is something that should be fairly obvious on physical exam.
Two other traumatic causes, uterine rupture and uterine inversion tend to be much more subtle.
Uterine Rupture
The patient for this will be a pregnant woman during her third trimester or presenting during labor.
The patient will have a history of a cesarean delivery or other surgery involving the uterus.
These patients will present with vaginal bleeding which would be consistent with postpartum hemorrhage.
However, the path of mnemonic finding and uterine rupture is a loss of fetal station. This is extremely high yield to understand and keep in mind.
The way that this will present in a vignette on an examination, is that the fetus will initially be at a particular fetal station, for example, at plus one or plus two, however, there will be a change in the fetal station to one of these lower or negative numbers such as minus one or minus two, indicating a loss of fetal station.
This is because as the fetus ruptures through the uterus, rather than progressing downward towards the cervix and the vagina towards a more positive fetal station, it will instead move in the opposite direction towards a more negative fetal station, thus resulting in a loss in fetal station.
Because the fetus is essentially rupturing through the uterus you may be able to palpate fetal parts during the abdominal exam on this particular patient. And therefore these two features the loss of fetal station, as well as the ability to palpate parts of the fetus on the abdominal exam, such as an arm or a leg are extremely classic for uterine rupture.
Pathophysiology
The pathophysiology of a uterine rupture is a tearing along the uterine scar during labor.
Therefore, it is secondary to the forces that are present during the contractions of labor.
These patients will typically have a previous uterine surgery, a prolonged course of labor, or may have high parity.
All of these different etiologies place increased stress on the uterus, ultimately resulting in uterine rupture.
Diagnosis
The diagnosis is going to be clinical as we look for the palpation of fetal parts, as well as a loss of fetal station.
Management
And as we can imagine, the fetus ripping through the uterus is going to be a medical emergency.
And therefore these patients need to be managed with a laparotomy as well as a cesarean delivery in order to remove the fetus.
Uterine Inversion
Our patient will present with sudden onset abdominal pain and vaginal bleeding.
The timing of this pain and vaginal bleeding is extremely critical as it occurs after traction on the umbilical cord.
In addition, we may also be able to appreciate a smooth round mass in the vagina after placental delivery.
Pathophysiology
The pathophysiology in the case of uterine inversion is excessive pressure on the umbilical cord. This will likely be present in the patient vignette on examinations.
Essentially, what is occurring here is that the placenta fails to detach from the uterine wall and therefore excessive pressure is made by the surgeon on the umbilical cord, ultimately resulting in uterine inversion.
Diagnosis
The diagnosis is going to be clinical.
On physical exam we should be able to appreciate that the uterus is not palpable in its usual position near the umbilicus, as it has been inverted from its usual position.
Management
- The first step in management in the case of uterine inversion is to manually replace the uterus.
- Following manual replacement of the uterus, we administer oxytocin. Because these patients often have excessive postpartum hemorrhage, we can also give IV fluids as well as a liter of blood if needed.
- If the patient is continuing to hemorrhage and we are having trouble replacing the uterus, then we can proceed with a laparotomy.
Below we have a schematic of the first step in the management of uterine inversion.

As shown here, the uterus has been inverted into a position that is far inferior to where it is supposed to be within the pelvic cavity.
We, therefore, apply pressure in an upward direction.
This ultimately allows us to replace the uterus to its usual position within the pelvic cavity.
Tissue
The two tissue causes of postpartum hemorrhage are Retained Placenta and Placenta Accreta, both of which are extremely high yield for examinations.
Retained Placenta
This is defined as a failure to deliver the placenta within 30 minutes of delivery of the fetus.
This, therefore, is going to occur during the third stage of labor.
Because the placenta is adhering still to the uterine wall, we are going to have excessive vaginal bleeding.
Pathophysiology
The underlying pathophysiology of a retained placenta is abnormal implantation of the placenta in the uterus and this has several high yield causes.
Risk factors
In order to understand what essentially leads up to a retained placenta, there are some key vocabulary terms that we will need to review.
These include:
- Placenta Accreta
- Placenta Increta
- Placenta Percreta.
In Placenta Accreta the placental villi adhere to the myometrium.
In Placenta Increta the placental villi implant into the myometrium.
This can be seen in the schematic below.

We can also have Placenta Percreta in which the placental villi penetrate into the myometrial wall.
Additional risk factors for a retained placenta are;
- Placenta Previa
- Fibroids
- Having a history of cesarean delivery or D&C.
Diagnosis
We can diagnose a retained placenta with an intrauterine manual exam in which we can appreciate that the placenta is still adherent to the uterus.
At this point, if we were to perform a pelvic ultrasound, we would be able to appreciate an echogenic mass or a Thickened Endometrial Stripe representing this retained placenta.
Management
The first step in the management of a retained placenta is to perform uterine massage and to administer in order to increase uterine tone and help the uterus to essentially expel the placenta from the pelvic cavity.
If these measures do not work, additional measures that we can utilize include:
- Manual removal of the placenta
- Performing a dilation and curettage (D&C)
- If the hemorrhage is severe and ongoing, we can perform an emergency hysterectomy
Regardless of which of these measures we use in order to remove the placenta, we should also perform a follow-up ultrasound to make sure that we removed all of the remaining placental tissue.
Placenta Accreta
The placental villi are adhering to the myometrium.
Placenta Accreta is an important risk factor for the development of a retained placenta.
However, this does not mean that Placenta Accreta always presents ultimately as post-partum hemorrhage in the context of a retained placenta as Placenta Accreta can be detected on an abnormal ultrasound during routine prenatal care.
However in the event that Placenta Accreta is not detected until delivery, then we may have a case of a retained placenta resulting in postpartum hemorrhage.
Pathophysiology
The pathophysiology of Placenta Accreta is the attachment of the placental villi directly to the myometrium as shown below.

Diagnosis
If Placenta Accreta is diagnosed prenatally, then a pelvic ultrasound will be able to appreciate villous lakes that are present in the placenta.
This finding of villous lakes is extremely high yield for examinations and is frequently how Placenta Accreta is tested.
An additional finding that may suggest Placenta Accreta is an irregularity or a blurring of the placenta myometrial border.
This blurring of the placenta myometrial border is consistent with our understanding that in this case the placenta villi are essentially adhering to the myometrium thus obscuring that border.
Management
In the event that we diagnose Placenta Accreta prenatally, then in terms of management, we should plan to perform a cesarean hysterectomy in which we perform a cesarean delivery and remove the uterus.
In doing so we will not have to deal with the consequences of a potential retained placenta which can ultimately result in life-threatening postpartum hemorrhage.
Thrombin
This refers to the various coagulopathies that can result in postpartum hemorrhage.
The most commonly tested is Von Willebrand Disease which presents in bleeding from mucosal sites. This can present with epistaxis menorrhagia or postpartum hemorrhage. However, it is likely that these patients will have a history in the patient vignette, menorrhagia, epistaxis, or some other sort of bleeding from mucosal sites.
© 2019 BoardsMD
Another important cause of postpartum hemorrhage in this discussion of coagulopathies is Disseminated Intravascular Coagulation (DIC).
There are several conditions which upon examinations in pregnant women in whom DIC has an increased risk of occurring, these include patients who have;
- Preeclampsia
- Amniotic Fluid Embolism
- HELLP Syndrome
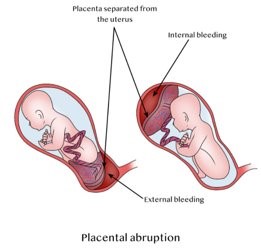
- Placental Abruption, which presents with painful third trimester bleeding.
There are several important causes of postpartum hemorrhage to keep in mind. But if we simply keep in mind the 4 T’s, including Tone, Trauma, Tissue, and Thrombin, we can help to organize these different causes and look for cues in the context of patient vignettes on examinations.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
