Preterm Labor
In this Module:
- Preterm Labor Risks to the Infant
- Braxton Hicks Contractions
- Fetal Fibronectin (FNN)
- Diagnosing Preterm Labor
- Managing Preterm Labor
- Tocolytics
- Magnesium Sulphate
- Predicting Preterm Labor
- Preventing Preterm Labor
High-yield topics related to preterm labor include:
- Risks to the Fetus Involved in Preterm Labor
- Braxton Hicks Contractions aka False Labor
- Diagnosis of Preterm labor
- Management of Preterm Labor
- Prevention of Preterm Labor
Preterm Labor Risks to the Infant
Question writers like to ask about preterm labor, its complications, diagnosis, prevention, and management. There's a good reason for this as there are significant risks to the fetus and ultimately the infant when it comes to preterm labor.
Preterm labor can increase the risk of:
- The Development of Neonatal Respiratory Distress Syndrome
- Bronchopulmonary Dysplasia (BPD)
- Retinopathy of Prematurity
- Necrotizing Enterocolitis.
- Patent Ductus Arteriosus
- Intraventricular Hemorrhage
With all these potential complications of preterm labor, we really need to be aware of how to diagnose, prevent, and manage preterm labor in our patients.
Braxton Hicks Contractions
In addition to being able to recognize and manage preterm labor, we must also be able to recognize conditions that may mimic preterm labor.
Also known as false labor, one classic presentation of false labor is with Braxton Hicks Contractions. This is something that frequently shows up on examinations.
©2019 BoardsMD
In Braxton Hicks Contractions our patient is going to be a pregnant woman who presents with irregular contractions, oftentimes with mild pain.
However, this is not a case of true labor. Instead, this is simply a result of the physiology of pregnancy and in particular dehydration.
Keep in mind that the uterus has a myometrial component which is made up of muscle. And if a pregnant patient becomes even mildly or moderately dehydrated, classically during the summer months, then that can ultimately cause a slight cramp in the muscle of the myometrium causing the uterus to contract.
This can result in these painful contractions. However, this is a case of false labor or Braxton Hicks Contractions rather than true labor.
Diagnosis
We can diagnose Braxton Hicks, contractions with the use of a speculum exam, as well as a fetal ultrasound. However, the real hallmark that will distinguish Braxton Hicks, contractions from true labor is that there will be no cervical change presence.
Therefore, these patients will have irregular contractions. Their pain will not be particularly severe, and they will have no cervical change.
Management
Once we determine that these patients are indeed experiencing false labor rather than true labor, we can simply reassure these patients and encourage them to hydrate in order to prevent future cramping of the myometrium and the resulting Braxton Hicks Contractions.
This is one of several reasons why we encourage patients to hydrate well during pregnancy.
Braxton Hicks vs. True Preterm Labor
During true preterm labor, the patient is going to be at less than 37 weeks.
This is the definition of preterm as after 37 weeks we are term and after 41 weeks we are considered to be post-term.
Unlike in Braxton Hicks Contractions, where a patient is presented with irregular and mildly painful contractions, in true preterm labor our patients will have regular painful contractions with increasing intensity. In addition, these patients also may present with some vaginal discharge, which will typically be either clear or with some tinting of blood.
Pathophysiology
There are multiple risk factors involved;
- History of preterm labor is a significant risk factor for the development of preterm labor.
- Having a short cervix is also a significant risk factor for preterm labor
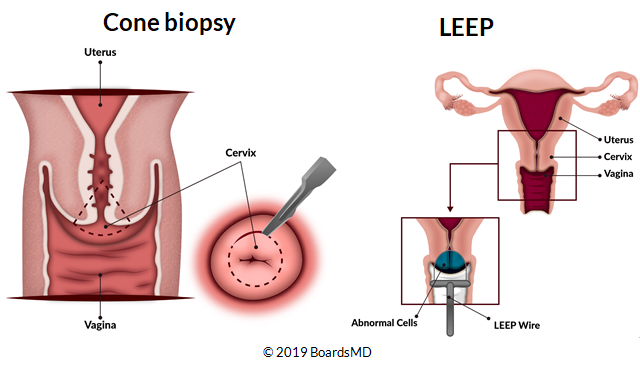
- Cervical procedures are also a significant risk factor. These surgical procedures include those that are used in terms of the diagnosis of cervical dysplasia including the cone biopsy as well as the LEEP procedure. we discuss both of these in more detail in our cervical dysplasia and cancer section.
Additional risk factors of the development of preterm labor include:
- Using amphetamines as well as smoking.
- Asymptomatic bacteriuria. We discussed this in more detail in our maternal infections lessons. However, this is why we treat asymptomatic bacteriuria in our pregnant patients in order to prevent these patients from developing preterm labor
- Inadequate maternal weight gain.
Fetal Fibronectin (FNN)
©2019 BoardsMD
Before we discuss the diagnosis and management of preterm labor in detail, we must first become familiar with Fetal Fibronectin (FFN)
Fetal Fibronectin is an extracellular matrix protein which ultimately binds together the uterus and the gestational sac. During labor when there are contractions, the uterus and the gestational sac essentially separate from one another.
This disturbs these extra cellular connections, ultimately causing levels of fetal fibronectin to rise. And therefore we can use this fetal fibronectin to help us determine whether the mother is going into labor. You must also understand how fetal fibronectin rises and falls throughout the pregnancy.
This is because there are high levels of fetal fibronectin in vaginal secretions during the first trimester. Levels of this protein than fall during the second and third trimester.
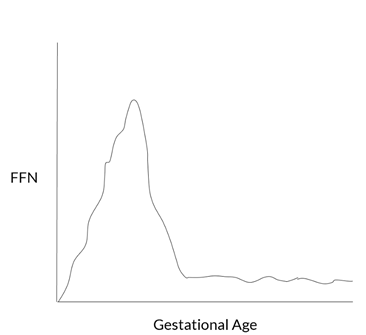
This protein will typically increase once again one to two weeks prior to labor, this can be appreciated by the schematic below where we can see that during the first trimester levels of fetal fibronectin will actually be quite high and therefore measuring fetal fibronectin during the first trimester is not very useful.
However, after approximately 22 weeks gestation levels of fetal fibronectin will remain relatively low. This will remain the case throughout the second and third trimesters.
Approximately one to two weeks prior to going into labor, the levels of fetal fibronectin will once again rise thus resulting in a positive fetal fibronectin test.
However, because fetal fibronectin is typically high up until approximately 22 weeks gestation, we typically only use this fetal fibronectin test between 22 and 34 weeks. If we have a negative fetal fibronectin test that we can determine that that patient is not going into labor.
However, if we have a positive fetal fibronectin test, then it is likely that that patient is going into labor, and this can be extremely useful in diagnosing preterm labor.
Diagnosing Preterm Labor
In order to diagnose preterm labor, the mother should have contractions that are of increasing frequency. Typically at least eight per hour.
In addition, as we discussed previously, unlike Braxton Hicks contractions patients with preterm labor will have cervical change.
For the purposes of examinations, cervical change is defined in this case as having cervical dilation greater than three centimeters or having effacement of the cervix.
If the patient is between 22 and 34 weeks gestation, then we could also use fetal fibronectin testing in order to help us to determine whether the patient is indeed going into preterm labor.
Managing Preterm Labor
The management can be quite complex as it depends on the gestational age.
If we break down the different components that go into managing these patients and then determine the patient's particular stage in terms of their gestational age, then we can simplify this greatly when it comes to how we answer these questions on examinations.
There are several key time points that you will see below.
©2019 BoardsMD
There are essentially three windows of time in terms of the gestational age into which our patient may fall which will determine how we manage her.
What you’ll note as we move forward in discussing this is that as we get earlier in terms of gestational age, meaning that the patient is more preterm, then we will essentially have to add on more agents.
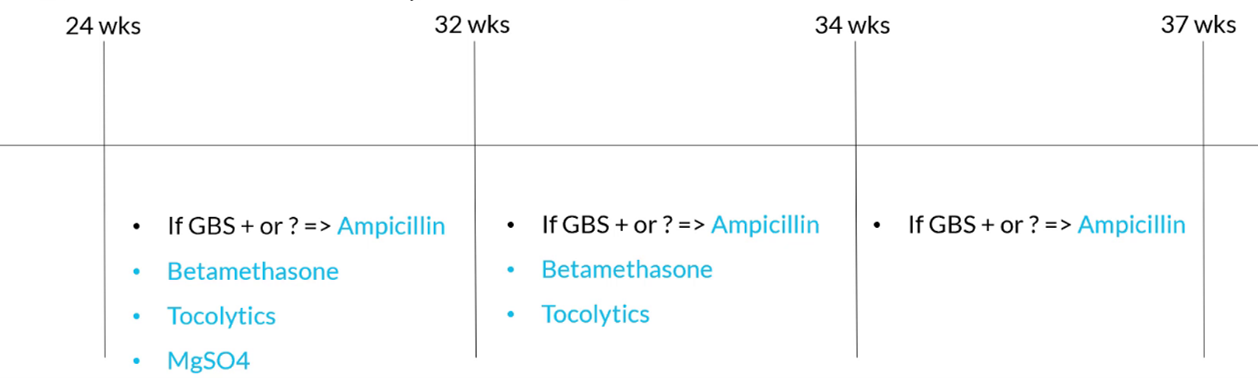
Between 34 and 37 Weeks
If our patient is between 34 and 37 weeks gestation and presents with preterm labor, If that patient is GBS positive, or we do not know the GBS status of that patient, then we can treat her with ampicillin.
Between 32 and 34 Weeks
If the patient is between 32 and 34 weeks gestation, then we can consider that patient to be more preterm than our previous patient. She will require additional agents.
Once again, if this patient is GBS positive or has an unknown GBS status, then we can treat her with intrapartum penicillin or ampicillin. Additionally, because we are dealing with potential delivery prior to 34 weeks gestation, we should also give this patient betamethasone in order to promote fetal lung maturity. We also treat patients in this time window with Tocolytics.
Between 24 and 32 Weeks
If our patient is between 24 and 32 weeks gestation, then this patient is considered to be more preterm than our previous two types of patients and therefore will require even more agents in terms of their management.
Once again, if the patient is GBS positive, or we do not know the GBS status of the patient, then we should treat her with intrapartum, ampicillin, or penicillin. Additionally, we will, once again, give betamethasone in order to promote fetal lung maturity and we also treat these patients with tocolytics.
One additional agent that we treat our patients with at prior to 32 weeks if they are going into preterm labor is magnesium sulfate as this helps to prevent the development of cerebral palsy.
As we move forward keep in mind that between 34 and 37 weeks, the most that we are going to treat our patient with in terms of preterm labor is ampicillin.
As our patient becomes more preterm, then we may need to add on betamethasone, tocolytics, or even magnesium sulfate.
If you simply start with our initial and most simple treatment method, then you can simply add on more agents as we get earlier and earlier into the pregnancy on board exam questions.
Recap of Preterm Labor Management
- We use ampicillin in patients who have unknown or positive GBS status in order to decrease the risk of GBS sepsis in the neonate
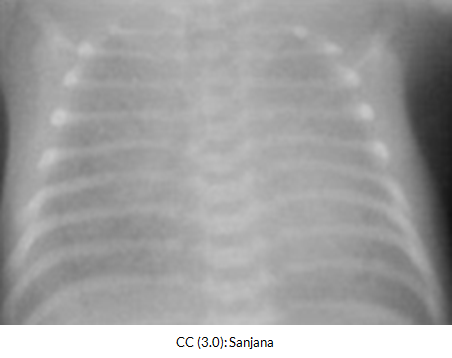
- We give betamethasone in preterm labor patients who are 24 to 34 weeks gestation. This helps to increase the production of surfactant and to promote fetal lung maturity, which ultimately helps to protect against the development of neonatal respiratory distress syndrome as shown in this chest x-ray below.
In this same group of patients between 24 and 34 weeks gestation who have developed preterm labor we also use tocolytics. This allows increased time for the betamethasone to take effect and to promote the development of the fetal lungs.
We give magnesium sulfate between 24 and 32 weeks gestation if our patient develops preterm labor as this helps to decrease the risk of cerebral palsy.
Tocolytics
A major role of Tocolytics is to give more time for betamethasone to take effect in our patients with preterm labor.
We have several options at our disposal when it comes to Tocolytics.
Each of these tocolytic agents has its own unique set of side effects.
Tocolytic agents include:
- indomethacin
- nifedipine
- terbutaline
- ritodrine
- magnesium sulfate (which is a weak tocolytic)
Because each of these agents has unique side effects, you must be aware of these potential adverse effects when distinguishing between the use of these different Tocolytics on examination questions.
- With the use of indomethacin, you should only use this at less than 32 weeks gestation as this is an end set, which has the potential to close the PDA.
- One of the key drawbacks of Nifedipine, which is a calcium channel blocker, is that a can cause hypotension and therefore it should be avoided in patients who have low blood pressure.
- With the Tocolytics terbutaline and ritodrine, these are both beta agonists and can ultimately cause increases in the patient's blood pressure. Therefore, both her terbutaline and ritodrine should be avoided in patients who have diabetes.
- With magnesium sulfate, which is a weak tocolytic, they should be avoided in patients with myasthenia gravis, as this has been shown to worsen symptoms in these patients.
Magnesium Sulphate
The indications for this agent include as seizure prophylaxis in patients who have eclampsia.
This is also used in patients who develop preterm labor at less than 32 weeks gestation as a measure to protect against the development of cerebral palsy.
In some patients, magnesium sulfate can accumulate to toxic levels. One of the first manifestations of this is a decrease in the deep tendon reflexes.
This is something that you often see on your OB/GYN rotation.
As you'll see the residents performing a mag check in order to check the patient's deep tendon reflexes.
As the levels of magnesium sulfate increase further, patients can also have a decrease in the respiratory rate as well as a decrease in cardiac conduction which can potentially be fatal.
Management of Magnesium Sulfate Toxicity
In order to manage magnesium sulfate toxicity, we first stop the magnesium sulfate and provide supportive measures.
And for patients, particularly those who are at risk of decreased cardiac conduction, you can also give IV calcium gluconate as a reversal agent.
Predicting Preterm Labor
Earlier in this module, we discussed several risk factors that are potent in the development of preterm labor.

Two major risk factors that help predict preterm labor:
- history of preterm labor in the past
- short cervix.
Evaluating Short Cervix
The method that we use to evaluate how short a patient cervix is, is with the use of an ultrasound during the second trimester.
This will generate a cervical length which you will likely see on examination questions.
In particular for patients who have no history of preterm labor in the past, they are considered to have a short cervix If their cervical length is less than or equal to two centimeters.
For patients who do have a history of preterm labor, then they are considered to have a short cervix that they have a cervical length of less than or equal to 2.5 centimeters.
The difference here is that if the patient has a history of preterm labor, then they are considered to have a short cervix even if the length of their cervix is 0.5 centimeters greater than a patient who has no history of preterm labor.
Commit these values to memory, as they will ultimately guide our management in terms of preventing preterm labor.
Preventing Preterm Labor
Because history of preterm labor, and having a short cervix are two major risk factors, here are really four major scenarios that we can generate from these two risk factors that will determine what we do in terms of preventing preterm labor.
In our first scenario, the patient will have no history of preterm labor. Additionally, her second trimester ultrasound shows that she has a normal cervix.
For this patient, she will simply resume normal follow-up. There is no need for any additional measure in order to prevent preterm labor in this relatively low risk patient
In our second scenario, our patient has no history of preterm labor. However, her second trimester ultrasound shows that she has a short cervix.
This would be defined as a patient who has a cervical length of two centimeters or less. In the case of this patient, we would manage her with progesterone in order to prevent her from developing preterm labor.
You can see here that in a patient with no history of preterm labor, whether she has a normal cervix or is determined to have a short cervix will ultimately result in two very different forms of management. Either:
- normal follow-up and routine prenatal care
- the use of progesterone to prevent the development of preterm labor.
scenario three and scenario four, in both of these cases, the patient will have a history of preterm labor.
And what you will see in both of these scenarios is that we should give intramuscular progesterone or progesterone injections to these patients in order to maintain the quiescence of the cervix.
For scenario three, we have a patient who has a history of preterm labor, however, her second trimester ultrasound shows that she has a normal cervical length. In this case, we administer intramuscular progesterone in order to prevent progression to preterm labor. We also perform serial ultrasounds of the cervix up until 24 weeks
In the fourth scenario, we once again, have a patient who is going to have a history of preterm labor. However, in this case, her second trimester ultrasound shows that she does indeed have a short cervical length.
In the case of a patient who has a history of preterm labor, this will be defined as having a cervical length that is less than 2.5 centimeters. In these patients who are considered to be at the highest risk for the development of preterm labor, we once again, give intramuscular progesterone.
Having a history of preterm labor, as well as a short cervix is an indication for placement of a cervical cerclage. And just like our patient in scenario three, who had a history of preterm labor, we should also perform serial ultrasound in these patients to continue to assess the cervical length up until 24 weeks gestation.
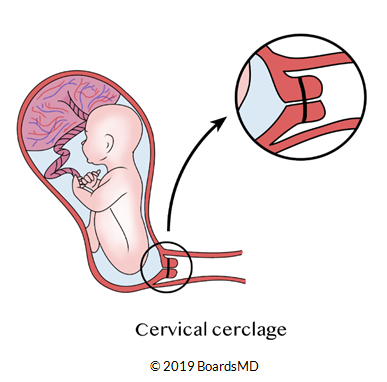
Below we have a schematic of a cervical cerclage.
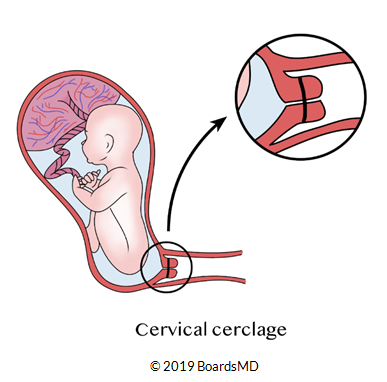
You can see here that we have the fetus present within the uterus. The cervix has been bound together using a band like material.
The idea of this band like material is that it essentially keeps the cervix shut closed so that even if this fetus pushes up against the cervix, it will remain shut against this pressure coming from the fetal head.
This cervical cerclage therefore will ultimately prevent this patient from progressing to preterm labor.
It is indicated in patients who have both a short cervix and a history of preterm labor in the past.
Cervical cerclage is reserved for our highest risk patients when it comes to preterm labor.

©2019 BoardsMD
In Conclusion
Now that we've discussed each of the four scenarios in detail in terms of the major risk factors for pre-term labor, let's go through each of these one last time in one united algorithm.
- You first must ask whether the patient has a history of preterm labor. If the patient does not have a history of preterm labor, then we proceed with a transvaginal ultrasound to assess the length of the cervix.
- If the length of the cervix is determined to be normal, then we can resume routine prenatal care. However, if the ultrasound reveals that the patient has a short cervix then we should administer vaginal progesterone in order to maintain the quiescence of the cervix.
- In the case of a patient who has no history of preterm labor, the definition of a short cervix is being less than or equal to two centimeters in length.
- However, if our patient does indeed have a history of preterm labor, we should perform a transvaginal ultrasound to assess cervical length. And for all patients who have the history of preterm labor, we can also give IM progesterone or progesterone injections.
- If the patient has a normal cervix, then we simply perform transvaginal ultrasound up until 24 weeks gestation.
- If the patient with a history of preterm labor has a short cervix, which in this case is defined as a cervical length less than or equal to 2.5 centimeters, then we can perform a cervical Cirque clause as well as transvaginal ultrasound up until 24 weeks gestation
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
